213
La Lettre du Cancérologue - volume XI - n° 6 - novembre-décembre 2002
CANCERS DIGESTIFS
CANCER COLORECTAL MÉTASTATIQUE
Les dérivés oraux du 5-FU
UFT
Les résultats définitifs de plusieurs études de phase III compa-
rant une fluoropyrimidine orale à un schéma de 5-FU en bolus
ont été publiés cette année. Deux études internationales paral-
lèles menées entre 1995 et 1997 ont comparé l’association
tégafur-uracil (UFT) et acide folinique (AF) à un schéma de
5-FU en bolus de type Mayo Clinic (5-FU bolus 425 mg/m2/j +
AF 20 mg/m2/j, 5 jours par mois). Dans les deux études, les
doses d’UFT étaient de 300 mg/m2/j associées à 90 mg/j d’AF,
28 jours sur 35.
Dans la première étude (1), 380 patients ont été inclus. Il n’y a
pas de différence significative en termes de survie sans pro-
gression (3,4 mois dans le bras UFT-AF et 3,3 mois dans le
bras 5-FU-AF). Les taux de réponse sont faibles : respective-
ment 10,5 % et 9 %. Enfin, la survie globale n’est pas non plus
significativement différente : 12,2 mois versus 10,3 mois.
Concernant la tolérance, l’UFT-AF a entraîné moins de
mucites de grades 3-4 (16 % au versus 2 %) et moins de neu-
tropénies de grades 3-4 (8 % versus 1 %). La deuxième étude
(2) a inclus 816 patients. Les résultats sont semblables à ceux
cités précédemment : pas de différence en termes de survie
globale (12,4 mois dans le bras UFT-AF, 13,4 mois dans le
bras Mayo Clinic), de survie sans progression (3,5 versus 3,8
mois), de taux de réponse (11,7 % versus 14,5 %). Les résul-
tats de la tolérance montrent également moins de mucites de
grades 3-4 et moins de neutropénies fébriles avec l’UFT-AF.
En conclusion, l’UFT-AF est moins toxique que le schéma
Mayo Clinic (moins de mucites et de neutropénies fébriles).
Cependant, le bras de référence comme le bras investigationnel
sont des traitements de première ligne insuffisants en termes
d’efficacité par rapport aux combinaisons associant du 5-FU
avec de l’oxaliplatine et du CPT11 et qui sont employées
actuellement. Cela ne fait que souligner les progrès qui ont été
effectués en quelques années, puisque la survie globale des
patients ayant un cancer colorectal métastatique a été doublée
par rapport aux résultats présentés dans ces études.
Éniluracil
Une autre étude a comparé l’association éniluracil et 5-FU au
schéma Mayo Clinic (3). L’éniluracil est un inhibiteur de la
dihydropyrimidine déshydrogénase. L’association d’éniluracil
et de 5-FU augmente la biodisponibilité orale du 5-FU, dimi-
nue sa clairance et ses variabilités pharmacocinétiques. L’asso-
ciation éniluracil-5-FU est administrée per os (éniluracil
11,5 mg/m2et 5-FU 1,15 mg/m2) tous les jours pendant
4semaines suivies d’une semaine de repos. Neuf cent quatre-
vingt-un patients ont été randomisés. Les résultats de survie
montrent une survie globale équivalente dans le bras éniluracil
et le bras Mayo Clinic (respectivement 13,3 versus 14,5 mois),
une survie sans progression inférieure dans le bras éniluracil
(20 semaines versus 22,7 semaines, p = 0,01) et un taux de
réponse similaire (12,2 % pour éniluracil et 12,7 % pour le
schéma Mayo Clinic). Moins de neutropénies de grades 3-4 et
de neutropénies fébriles sont présentes avec l’éniluracil (5 et
0,2 % contre 47 % et 9,4 %). Les nausées et les mucites sont
également moins fréquentes.
Capécitabine
La capécitabine fait également partie des fluoropyrimidines
orales. Elle a la particularité d’être métabolisée en 5-FU, prin-
cipalement au niveau de la cellule tumorale. Cette propriété est
intéressante puisque, en théorie, la capécitabine permettrait
d’augmenter la dose d’intensité de 5-FU en réduisant les effets
secondaires systémiques. L’étude menée par le Xeloda Colo-
rectal Cancer Study Group a comparé la capécitabine
(1 250 mg/m2x 2/j J1 à J14 toutes les 3 semaines) au schéma
FUFOL Mayo Clinic chez des patients en première ligne méta-
statique (4). En 16 mois, sur 59 centres, 602 patients ont été
inclus dans l’étude. Il faut souligner qu’il n’y avait pas de
limite supérieure d’âge et que l’âge médian des patients était
de 64 ans (groupe capécitabine) et de 63,5 ans (groupe Mayo
Clinic), les extrêmes étant, respectivement, de 84 et 86 ans.
L’objectif principal était le taux de réponse : 18,9 % dans le
bras capécitabine et 15 % dans le bras Mayo Clinic. Les temps
jusqu’à progression n’étaient pas significativement différents :
respectivement 5,2 mois et 4,7 mois. Enfin, les médianes de
survie globale sont équivalentes : 13,2 mois versus 12,1 mois.
Le profil de tolérance est différent dans les deux groupes : le
schéma Mayo Clinic entraîne davantage de mucites de grades
3-4 (13 % versus 1 %), d’alopécies et de neutropénies de
Prise en charge des cancers digestifs :
avancées diagnostiques et thérapeutiques en 2002
● C. Tournigand*
* Hôpital Saint-Antoine, Paris.

214
La Lettre du Cancérologue - volume XI - n° 6 - novembre-décembre 2002
grades 3-4 (20 % versus 2 %). En revanche, la capécitabine
entraîne plus de syndromes mains-pieds de grades 3-4 (16,2 %
versus 0,3 %). L’incidence des diarrhées est équivalente dans
les deux bras (environ 10 % de grades 3-4). Les résultats de
cette étude sont à mettre en parallèle avec ceux de l’étude amé-
ricaine bâtie sur le même mode (5). Les taux de réponse
étaient plus élevés dans le bras capécitabine mais il s’agissait
de réponses investigateurs, non revues par un panel d’experts.
Les autres conclusions sont équivalentes à celles de l’étude
présentée précédemment.
Une étude européenne s’est intéressée à la préférence des
patients entre un traitement par UFT-LV per os à domicile et
un traitement de type Mayo Clinic (6). Les patients recevaient
leur première cure selon l’un ou l’autre protocole (i.v. ou per
os) puis passaient à l’autre voie d’administration lors de la
deuxième cure. Pour la suite, ils pouvaient choisir la voie
d’administration qu’ils préféraient. L’effectif de patients était
faible : 38 patients au total. Un questionnaire avant le début du
traitement montrait que les critères de choix de l’un ou l’autre
des traitements seraient essentiellement des critères de tolé-
rance : la préférence irait au traitement qui donnerait le moins
de risque d’infection, de nausées, de vomissements ou de diar-
rhées. Les critères de “traitement à domicile” ou de “traitement
per os” venaient seulement en 4eet 6eposition, respectivement.
Après la deuxième cure (les patients avaient donc testé les
deux voies d’administration), le critère de “traitement à domi-
cile” devenait le plus important. Globalement, 84 % des
patients préféraient le traitement par voie orale.
De l’ensemble de ces résultats concernant les fluoropyrimi-
dines orales, on peut retenir qu’elles ont une activité compa-
rable à celle du 5-FU en bolus, avec une toxicité moindre et
une plus grande facilité d’utilisation pour les patients. Cepen-
dant, il faut remarquer, à l’instar des éditorialistes du Journal
of Clinical Oncology, que le FUFOL Mayo Clinic est plus
toxique que le 5-FU administré en perfusion continue. Or, il
n’y a pas, à l’heure actuelle, d’étude comparant un schéma de
5-FU continu à une fluoropyrimidine orale. Enfin, le 5-FU
(oral ou i.v.) en monothérapie n’est pas actuellement le traite-
ment de choix en première ligne métastatique, compte tenu des
bons résultats obtenus grâce aux associations avec l’oxalipla-
tine et le CPT11. Les fluoropyrimidines orales devront donc
être testées en combinaison avec l’une ou l’autre de ces molé-
cules, ce qui imposera au patient une hospitalisation pour rece-
voir celles-ci par voie veineuse.
Chimiothérapie intra-artérielle
Les résultats définitifs de l’étude intergroupe du SWOG et de
l’ECOG ont été publiés par M. Kemeny (7). Il s’agit d’une
étude randomisée comparant, chez des patients ayant un cancer
colorectal avec une à trois métastases hépatiques, une sur-
veillance à un traitement par chimiothérapie intra-artérielle
associée à du 5-FU i.v. continu. Les premiers résultats avaient
été présentés à l’ASCO en 1999. Le groupe traité recevait du
FUDR 4 à 8 semaines après l’intervention, à la dose de
0,1 mg/kg/j pendant 14 jours tous les 28 jours. Quatre cycles,
au maximum, étaient administrés. Les doses de 5-FU continu
étaient de 200 mg/m2/j sur 14 jours en même temps que la chi-
miothérapie intra-artérielle. Après la fin de la chimiothérapie
intra-artérielle, 8 cycles supplémentaires de 5-FU étaient admi-
nistrés (300 mg/m2/j). L’âge médian était de 62 ans dans le
groupe contrôle et de 59 ans dans le groupe chimiothérapie.
Dans plus de 75 % des cas, les patients avaient un indice de
performance de 0. Les taux de rechute observés à 4 ans sont de
25 % dans le groupe contrôle et de 46 % dans le groupe
chimiothérapie (p = 0,04). La survie sans rechute hépatique
était, respectivement, de 43 % et 67 % (p = 0,03). La survie
globale, quant à elle, n’est pas significativement différente :
49 mois dans le groupe contrôle, 63,7 mois dans le groupe chi-
miothérapie (p = 0,6), mais l’essai n’était pas dimensionné
pour répondre à la question. Cette étude confirme que la chi-
miothérapie intra-artérielle permet un meilleur contrôle local
hépatique mais qu’il s’agit d’une technique difficile, même
entre des mains entraînées (100 patients inclus dans cette étude
en 6,5 ans).
Parmi les résultats importants rapportés cette année figurent
ceux de l’essai N 9741 du NCCTG (8). Sur les six bras initiaux
de cette étude de première ligne métastatique, trois bras
avaient été fermés en mars 2000 en raison de la toxicité
(schéma Mayo Clinic, Mayo Clinic + oxaliplatine, Mayo Cli-
nic + CPT11). Restaient alors le schéma dit “de Saltz” (IFL,
CPT11 + 5-FU en bolus), le schéma FOLFOX 4 et le schéma
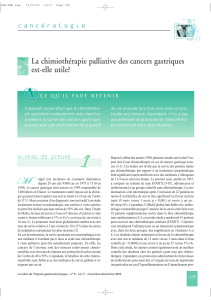
associant oxaliplatine et CPT11. Les résultats montrent que le
schéma FOLFOX 4 est supérieur au schéma IFL en termes de
survie sans progression, de survie globale et de taux de
réponse (tableau II). En dehors des neuropathies, le schéma
CANCERS DIGESTIFS
Référence n Taux de SSP SG
réponse (%)
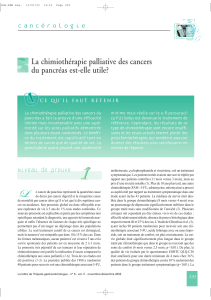
(1) UFT 190 10,5 3,4 mois 12,2 mois
Mayo Clinic 190 9 3,3 mois 10,3 mois
(2) UFT 409 11,7 3,5 mois 12,4 mois
Mayo Clinic 407 14,5 3,8 mois 13,4 mois
(3) Éniluracil 485 12,2 20 semaines 13,3 mois
Mayo Clinic 479 12,7 22,7 semaines 14,5 mois
(4) Capécitabine 301 18,9 5,2 mois 13,2 mois
Mayo Clinic 301 15 4,7 mois 12,1 mois
(5) Capécitabine 302 25,8 4,3 mois 12,5 mois
Mayo clinic 303 11,6 4,7 mois 13,3 mois
Tableau I. Fluoropyrimidines orales : essais randomisés.
SSP : survie sans progression ; SG : survie globale.
IFL FOLFOX 4 Oxali-CPT11
RO 29 % 38 % 28 %
p (vs IFL) – 0,03 0,89
SSP 6,9 8,8 6,7
p (vs IFL) – 0,0009 > 0,5
SG 14,1 18,6 16,5
Survie à 1 an 58 % 71 % 65 %
p (vs IFL) – 0,002 immature
Tableau II. Étude N 9741 : 5-FU/AF et oxaliplatine ou CPT11 ou oxa-
liplatine-CPT11 (8). Efficacité globale.

215
La Lettre du Cancérologue - volume XI - n° 6 - novembre-décembre 2002
FOLFOX 4 est également mieux toléré que le schéma IFL. Ces
résultats ont été à l’origine d’une démarche accélérée de la
FDA pour que l’oxaliplatine soit enfin disponible aux États-
Unis.
Traitement adjuvant du cancer du côlon
Edrecolomab
C’est dans la revue Lancet que sont parus des résultats de
l’étude comparant edrecolomab (anticorps 17-1-A) seul, edre-
colomab + 5-FU-AF et 5-FU-AF (9). Plus de 900 patients
ayant un cancer du côlon de stade III ont été randomisés.
Après un suivi médian de 26 mois, la survie globale à 3 ans de
la combinaison anticorps et chimiothérapie n’était pas diffé-
rente de celle sous chimiothérapie seule (74,7 % versus
76,1 %). La survie sans progression était significativement
plus courte avec l’edrecolomab seul par rapport à la chimiothé-
rapie (53 % versus 65,5 %). Dans cette étude, l’anticorps 17-1-A
en adjuvant n’apporte donc pas de bénéfice par rapport à une
chimiothérapie dans les cancers du côlon de stade III.
Les résultats de l’étude américaine, en revanche, sont en
faveur de l’edrecolomab (10). Cette étude de phase III compa-
rait le schéma FUFOL Mayo Clinic 6 mois et l’association
5-FU lévamisole 12 mois, avec ou sans edrecolomab. La sur-
vie globale à 3 ans est de 81,6 % dans le bras avec l’anticorps
et de 78,9 % dans le bras sans anticorps. Cette différence est
statistiquement significative. En revanche, la survie sans
rechute n’est pas différente (66,6 % versus 67,5 %). Les résul-
tats définitifs seront à analyser de près.
LV5FU2
Toujours en adjuvant, chez les patients ayant un cancer du
côlon de stade II ou III, citons les résultats de l’essai du GER-
COR qui valide le LV5FU2 en adjuvant (11). Il s’agit d’une
étude bâtie sur une double randomisation entre LV5FU2 et
FUFOL (AF 200 mg/m2, 5-FU 400 mg/m2en bolus de J1 à J5
toutes les 4 semaines), d’une part, et 24 versus 36 semaines,
d’autre part. Les premiers résultats montrent que la survie sans
progression est identique entre 24 et 36 semaines de traitement.
La survie sans rechute n’est pas significativement différente
entre FUFOL et LV5FU2, mais les toxicités de grades 3-4 sont
moins fréquentes avec LV5FU2. En termes de survie globale,
il n’y a pas de différence entre les deux schémas ni entre les
deux durées du traitement adjuvant. Cette étude valide donc le
schéma LV5FU2 en adjuvant pendant 6 mois.
Sujets âgés
La chimiothérapie adjuvante chez les sujets âgés apporte-t-elle
le même bénéfice en survie que chez les sujets plus jeunes ?
C’est la question à laquelle deux études américaines ont tenté
de répondre, selon des méthodologies différentes. La première
étude a repris les données de 7 essais de phase III
(3 351 patients) qui avaient comparé une chimiothérapie adju-
vante par 5-FU et lévamisole ou acide folinique à la chirurgie
seule dans les stade II et III (12). Les auteurs ont analysé le
bénéfice en survie selon les groupes d’âge ( 50 ans, 51-60 ans,
61-70 ans, > 70 ans). Ils retrouvent un bénéfice en survie simi-
laire, quelle que soit la catégorie d’âge du patient. Par ailleurs,
les effets secondaires n’ont pas été plus fréquents chez les
malades de plus de 70 ans. La deuxième étude est une étude de
cohorte prospective non randomisée (3 357 patients) réalisée à
partir d’une base de données (SEER) (13). La survie des
patients de stade III dont l’âge était supérieur à 67 ans a été
comparée entre pas de traitement adjuvant et une chimiothéra-
pie adjuvante à base de 5-FU. Les résultats montrent que le
5-FU diminue le risque de décès de 27 %. La survie à 5 ans est
de 52,7 % dans le bras traité et de 40,7 % dans le bras non
traité.
CANCERS DU PANCRÉAS
Maladie localement avancée ou métastatique
Il faut souligner cette année le nombre important d’études de
phase III publiées sur le cancer du pancréas avancé : au moins
quatre études randomisées incluant un total de près de
900 patients. Cela montre le dynamisme des différentes
équipes dans ce domaine.
L’étude américaine de Berlin et al. a comparé la gemcitabine à
l’association gemcitabine et 5-FU (14). Les études de phase II
gemcitabine-5-FU avaient montré des résultats variables avec
des survies globales entre 7 et 11 mois, selon les schémas utili-
sés et les caractéristiques des patients inclus. Les schémas de
cette étude randomisée étaient soit la gemcitabine à
1000 mg/m2/semaine, 3 semaines sur 4, soit l’association de
gemcitabine (même schéma) et de 5-FU en bolus de
600 mg/m2/semaine, également 3 semaines sur 4. Trois cent
vingt-sept patients ont été inclus dans les deux bras, avec une
majorité de patients métastatiques (environ 90 % dans chaque
bras). Les médianes de survie globale ne sont pas significative-
ment différentes : 5,4 mois dans le bras gemcitabine seule,
6,7 mois dans le bras gemcitabine et 5-FU. Il en est de même
pour la survie sans progression (2,2 mois versus 3,4 mois). Les
taux de réponse sont très faibles dans les deux bras : 5,6 %
versus 6,9 %. Même si l’incidence de toxicités de grades 3-4
est plus importante dans le bras gemcitabine-5-FU, les diffé-
rences ne sont pas significatives. Il s’agit principalement de
toxicités digestives et hématologiques (neutropénies). En
conclusion, l’adjonction de 5-FU en bolus ne semble pas amé-
liorer les résultats de la gemcitabine administrée en
30 minutes.
Une étude italienne a comparé la gemcitabine seule à l’asso-
ciation gemcitabine-cisplatine (15). La gemcitabine était admi-
nistrée dans les deux bras en perfusion de 1 000 mg/m2sur
30 minutes toutes les semaines, 7 semaines de suite, suivies
d’une pause de 2 semaines puis de 2 cycles de 6 semaines. Le
cisplatine était délivré à la dose de 25 mg/m2par semaine,
avant chaque perfusion de gemcitabine (sauf à J22). Les
patients avaient une maladie localement avancée ou métasta-
tique bien équilibrée dans les deux bras. Les taux de réponse
ont été, respectivement de 9,2 % et de 26,4 % (p = 0,02). Les
survies sans progression sont de 8 semaines versus 20 semaines,
la différence étant significative (p = 0,48). En revanche, la
survie globale n’est pas significativement différente dans les
deux bras (20 versus 30 semaines). En termes de tolérance, la
seule différence a été l’asthénie, plus fréquente dans le bras

216
La Lettre du Cancérologue - volume XI - n° 6 - novembre-décembre 2002
avec cisplatine (24 % contre 9 % avec la gemcitabine seule).
Ces résultats sont donc en faveur d’une association de gemci-
tabine avec un dérivé du platine par rapport à la gemcitabine
en monothérapie.
L’intérêt du marimastat a été testé dans les cancers du pan-
créas avancés en comparant gemcitabine-placebo à gemcita-
bine-marimastat (16). Le marimastat est un inhibiteur des
métalloprotéinases, enzymes responsables de la dégradation de
la matrice extracellulaire, favorisant l’invasion tumorale. Le
marimastat n’a pas un effet cytotoxique, mais son action
consiste en une inhibition de la croissance cellulaire et du
potentiel métastatique des cellules tumorales. Dans cet essai
randomisé, la gemcitabine était administrée selon un schéma
hebdomadaire de 1 000 mg/m2en 30 minutes. Le marimastat
était administré oralement à la dose de 10 mg deux fois par
jour. Le nombre de patients inclus a été de 239. Il n’a pas été
mis en évidence de différence de survie globale (médiane de
165 jours dans le bras gemcitabine-marimastat et de 164 jours
dans le bras gemcitabine-placebo). Les taux de réponse ont été,
respectivement, de 11 % et 16 %. La survie sans progression
est également équivalente dans les deux bras. La toxicité la
plus fréquente du marimastat consiste en des douleurs
musculosquelettiques, résolutives lors de l’interruption du trai-
tement. Cet effet secondaire a touché 59 % des patients sous
marimastat, 4 % ayant une toxicité de grade 3 ou 4. Le mari-
mastat n’augmente donc pas l’efficacité de la gemcitabine. Ce
type d’étude n’est sans doute pas la meilleure façon d’évaluer
l’effet de telles molécules qui ont des mécanismes d’action dif-
férents des cytotoxiques habituels, probablement plus efficaces
lorsque le contingent tumoral est plus faible.
Une équipe anglaise a randomisé le 5-FU en perfusion conti-
nue 300 mg/m2/jour associé ou non à la mitomycine hebdoma-
daire (17). Deux cent huit patients ont été inclus. Les résultats
sont semblables à ceux présentés en 2001 à l’ASCO : le taux
de réponse a été significativement plus élevé dans le bras com-
biné (17,6 % versus 8,4 %), mais la réponse symptomatique, la
médiane de survie sans progression (3,8 mois versus 2,8 mois)
et la médiane de survie globale (6,5 mois versus 5,1) ne diffè-
rent pas significativement.
Traitement adjuvant
L’étude ESPAC, dont les résultats avaient été présentés à
l’ASCO en 2000, a été publiée en 2001 (18). Il s’agit d’une
étude randomisée en situation adjuvante, qui cherchait à définir
les rôles respectifs de la radio-chimiothérapie (45 Gy + 5-FU)
et de la chimiothérapie (5-FU et acide folinique en bolus heb-
domadaire). Certains patients ont été inclus dans une étude
factorielle à 2 x 2 bras (observation, RT-CT, CT, RT-CT et
CT), alors que d’autres patients ont été randomisés entre
observation et CT, et d’autres, enfin, entre observation et RT-
CT. La complexité de l’étude rend l’analyse délicate, mais les
résultats indiquent que la radio-chimiothérapie ne semble pas
augmenter significativement la survie. En revanche, la survie
médiane des patients ayant reçu une chimiothérapie adjuvante
est significativement plus longue que celle des patients n’en
ayant pas reçu (19,7 mois versus 14 mois, p = 0,0005).
CANCERS DE L’ESTOMAC ET DE L’ŒSOPHAGE
Une étude multicentrique anglaise a porté sur 369 patients qui
ont reçu en double aveugle soit du marimastat à la dose de
10 mg x 2 par jour pendant une durée théorique de 18 mois,
soit un placebo (19). La population étudiée comportait un
mélange de patients non prétraités et de patients ayant reçu
auparavant une ligne de chimiothérapie à base de 5-FU sans
signe de progression sous ce schéma. Environ un tiers des
patients avaient déjà reçu une chimiothérapie. Il s’agissait de
patients en bon état général (indice de performance 0 ou 1). La
majorité des patients avaient des métastases (respectivement,
71 % et 73 %). La survie sans progression est en faveur du
groupe marimastat (p = 0,043). La médiane de survie du
groupe marimastat est légèrement supérieure à celle du groupe
placebo (160 jours versus 138 jours, p = 0,028). Le pourcen-
tage de patients vivant à 2 ans est, respectivement, de 9 % et
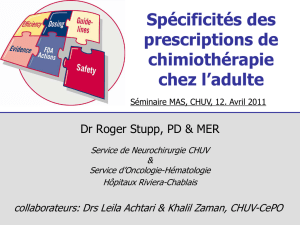
de 3 % (p = 0,12). L’analyse par sous-groupe indique que la
différence de survie globale est significative en faveur du
marimastat pour les patients ayant déjà reçu une chimiothéra-
pie antérieurement : 253 versus 175 jours (p = 0,006)
(figure 1). Il s’agit de la première étude d’envergure dans les
cancers digestifs évaluant l’effet d’un inhibiteur des métallo-
protéinases. Si certaines données sont encourageantes, il faut
certainement retenir que ce type de traitement en monothérapie
chez des patients avec maladie avancée n’est pas satisfaisant,
car si la médiane de survie est supérieure pour le marimastat
par rapport au placebo, elle n’est que de 160 jours, soit à peine
plus de 5 mois, et donc largement inférieure à ce qui est obtenu
avec une chimiothérapie conventionnelle.
Toujours en situation métastatique, une comparaison entre le
schéma ECF (épirubicine 50 mg/m2, cisplatine 60 mg/m2et
5-FU continu 200 mg/m2/j) et le MCF (mitomycine 7 mg/m2,
cisplatine 60 mg/m2et 5-FU continu 300 mg/m2) a été effec-
tuée chez des patients ayant un cancer de l’œsophage ou de
l’estomac avancé (20). Cette étude avait été menée à la suite
des travaux montrant la supériorité de l’ECF sur le schéma
FAMTX. Les taux de réponse sont de 42,4 % avec l’ECF
(289 patients) et de 44,1 % (285 patients) avec le MCF, cette
différence n’étant pas significative. La survie sans progression
est de 7 mois dans les deux bras, la survie globale médiane est
de 9,4 mois pour l’ECF et de 8,7 mois pour le MCF. En termes
CANCERS DIGESTIFS
1
0,8
0,6
0,4
0,2
0
Années
Marimastat (n = 61) médiane = 253 jours
Placebo (n = 62) médiane = 175 jours
Hazard ratio = 1,68 (1,16-2,44)
p = 0,006
Survival estimate
0123
4
Figure 1. Survie globale (sous-groupe chimiothérapie).

217
La Lettre du Cancérologue - volume XI - n° 6 - novembre-décembre 2002
de tolérance, l’ECF entraîne davantage de neutropénies de
grades 3-4 et d’alopécies de grade 2, alors que le MCF donne
plus de thrombopénies et de syndromes mains-pieds. L’ana-
lyse de la qualité de vie (QLQC30) est en faveur du schéma
ECF. Cette étude montre que le schéma ECF reste un des stan-
dards dans cette indication. ■
RÉFÉRENCES BIBLIOGRAPHIQUES
1. Carmichael J, Popiela T, Radstone D et al. Randomized comparative study of
tegafur/uracil and oral leucovorin versus parenteral fluorouracil and leucovorin in patients
with previously untreated metastatic colorectal cancer. J Clin Oncol 2002 ; 20 (17) : 3617-27.
2. Douillard JY, Hoff PM, Skillings JR et al. Multicenter phase III study of uracil/tegafur
and oral leucovorin versus fluorouracil and leucovorin in patients with previously untreated
metastatic colorectal cancer. J Clin Oncol 2002 ; 20 (17) : 3605-16.
3. Schilsky RL, Levin J, West WH et al. Randomized, open-label, phase III study of a 28-day
oral regimen of eniluracil plus fluorouracil versus intravenous fluorouracil plus leucovorin
as first-line therapy in patients with metastatic/advanced colorectal cancer. J Clin Oncol
2002 ; 20 (6) : 1519-26.
4. Van Cutsem E, Twelves C, Cassidy J et al. Oral capecitabine compared with intravenous
fluorouracil plus leucovorin in patients with metastatic colorectal cancer : results of a
large phase III study. J Clin Oncol 2001 ; 19 (21) : 4097-106.
5. Hoff PM, Ansari R, Batist G et al. Comparison of oral capecitabine versus intravenous
fluorouracil plus leucovorin as first-line treatment in 605 patients with metastatic colorec-
tal cancer : results of a randomized phase III study. J Clin Oncol 2001 ; 19 : 2282-92.
6. Borner MM, Schoffski P, de Wit R et al. Patient preference and pharmacokinetics of oral
modulated UFT versus intravenous fluorouracil and leucovorin : a randomised crossover
trial in advanced colorectal cancer. Eur J Cancer 2002 ; 38 (3) : 349-58.
7. Kemeny MM, Adak S, Gray B et al. Combined-modality treatment for resectable metas-
tatic colorectal carcinoma to the liver : surgical resection of hepatic metastases in combi-
nation with continuous infusion of chemotherapy, an intergroup study. J Clin Oncol 2002 ;
20 (6) : 1499-5052.
8. Goldberg RM, Morton RF, Sargent DJ et al. N 9741 : oxaliplatin or CPT11 + 5-fluorou-
racil/leucovorin or oxaliplatin + CPT11 in advanced colorectal cancer. Initial toxicity and
response data from a GI Intergroup study. Proc ASCO, 2002 abstr. 511.
9. Punt CJ, Nagy A, Douillard JY et al. Edrecolomab alone or in combination with fluorou-
racil and folinic acid in the adjuvant treatment of stage III colon cancer : a randomised
study. Lancet 2002 ; 360 (9334) : 671-7.
10. Anthony L Fields, Alan M Keller, Lee Schwartzberg et al. Edrecolomab (17-1-A anti-
body) in combination with 5-fluorouracil (FU) based chemotherapy in the adjuvant treat-
ment of stage III colon cancer : results of a randomised North American phase III study.
Proc ASCO 2002 ; abstr. 508.
11. Andre T, Colin P, Louvet C et al. Phase III trial (GERCOR C96.1) comparing
bimonthly LV5FU2 to monthly 5FU-leucovorin high dose in patients with Dukes B2 and C
colon cancer. Proc ASCO 2002, abstr. 529
12. Sargent DJ, Goldberg RM, Jacobson SD et al. A pooled analysis of adjuvant chemothe-
rapy for resected colon cancer in elderly patients. N Engl J Med 2001 ; 345 (15) : 1091-7.
13. Iwashyna TJ, Lamont EB. Effectiveness of adjuvant fluorouracil in clinical practice : a
population-based cohort study of elderly patients with stage III colon cancer.
J Clin Oncol 2002 ; 20 (19) : 3992-8.
14. Berlin JD, Catalano P, Thomas JP. Phase III study of gemcitabine in combination with
fluorouracil versus gemcitabine alone in patients with advanced pancreatic carcinoma :
Eastern Cooperative Oncology Group Trial E2297. J Clin Oncol 2002 ; 20 (15) : 3270-5.
15. Colucci G, Giuliani F, Gebbia V et al. Gemcitabine alone or with cisplatin for the
treatment of patients with locally advanced and/or metastatic pancreatic carcinoma : a
prospective, randomized phase III study of the Gruppo Oncologia dell’Italia Meridionale.
Cancer 2002 ; 94 (4) : 902-10.
16. Bramhall SR, Schulz J, Nemunaitis J et al. A double-blind placebo-controlled, rando-
mised study comparing gemcitabine and marimastat with gemcitabine and placebo as first
line therapy in patients with advanced pancreatic cancer. Br J Cancer 2002 ; 87 (2) : 161-7.
17. Maisey N, Chau I, Cunningham D et al. Multicenter randomized phase III trial compa-
ring protracted venous infusion (p.v.i.) fluorouracil (5-FU) with p.v.i. 5-FU plus mitomycin
in inoperable pancreatic cancer. J Clin Oncol 2002 ; 20 (14) : 3130-6.
18. Neoptolemos JP, Dunn JA, Stocken DD et al. Adjuvant chemoradiotherapy and chemo-
therapy in resectable pancreatic cancer : a randomised controlled trial. Lancet 2001 ; 358
(9293) : 1576-85.
19.Bramhall SR, Hallissey MT, Whiting J et al. Marimastat as maintenance therapy for patients
with advanced gastric cancer : a randomised trial. Br J Cancer 2002 ; 86 (12) : 1864-70.
20. Ross P, Nicolson M, Cunningham D et al. Prospective randomized trial comparing
mitomycin, cisplatin, and protracted venous-infusion fluorouracil (p.v.i. 5-FU) with epiru-
bicin, cisplatin, and p.v.i. 5-FU in advanced oesophagogastric cancer. J Clin Oncol 2002 ;
20 (8) : 1996-2004.
L’avenir
de la chimiothérapie
en dérivés oraux
* Unité de gastroentérologie,
Institut Custave-Roussy, Villejuif
Deux molécules de chimio-
thérapie analogues oraux
du 5-FU, la capécitabine et
l’UFT ont été récemment
mis sur le marché. Le
mécanisme d’action de ces
molécules est différent
puisque la capécitabine est
une prodrogue du 5-FU
absorbé et subissant des
étapes métaboliques
l’amenant à la transforma-
tion en 5-FU au sein de la
cellule tumorale. L’UFT est
une combinaison d’une
prodrogue du 5-FU le ftora-
fur et d’uracile qui inhibe la
principale enzyme de cata-
bolisme du 5-FU. Il est déjà
acquis que ces deux molé-
cules ont une activité dans
le cancer colorectal méta-
stasé. De grandes études
de phase III ont montré
qu’elles étaient, en mono-
chimiothérapie, d’efficacité
comparable à un schéma
de référence américain le
5-FU + acide folinique de la
Mayo Clinic. La différence
se fait plutôt en termes de
toxicité, les chimiothéra-
pies orales étant moins
toxiques en plus de leur
facilité d’utilisation. Il s’agit
cependant d’études de
monochimiothérapie et la
comparaison n’est pas
faite versus des schémas
de perfusion continue de 5-
FU dont on sait qu’ils sont
plus actifs et mieux tolérés.
Il n’existe pas à ce jour de
comparaison directe entre
ces deux nouveaux agents,
la différence entre les deux
se faisant plutôt au niveau
de la toxicité : plus de syn-
dromes main-pied avec la
capécitabine et plus de
diarrhée avec l’UFT. C’est
au sein des associations
que ces molécules ont le
plus grand intérêt que ce
soit en association avec
l’irinotécan, l’oxaliplatine
ou la radiothérapie. Des
schémas d’association ont
déjà fait preuve d’une effi-
cacité prometteuse leur
permettant de menacer
l’équivalent intraveineux,
au premier rang se situent
les deux associations
capécitabine oxaliplatine
et capécitabine-irinotécan.
Il est tout à fait possible
que les études de phase III
à venir permettent de
démontrer que le 5-FU tra-
ditionnel n’a plus sa place
dans le traitement du can-
cer colorectal ce qui serait
une révolution. Le schéma
capécitabine-oxaliplatine-
radiothérapie est égale-
ment un protocole promet-
teur dans le traitement du
cancer du rectum. Le
champ d’action des fluoro-
pyrimidines orales ne se
limite pas là puisque nous
disposons déjà de résul-
tats préliminaires d’une
étude randomisée britan-
nique suggérant qu’il est
possible de remplacer le 5-
FU en perfusion continue
du très contraignant
schéma ECF (5-FU perfu-
sion continue pendant
21 semaines) lors du trai-
tement des cancers gas-
triques métastasés. Il est
donc raisonnable d’envisa-
ger dans les 5 ans à venir
la disparition complète des
indications de 5-FU en per-
fusion au profit des molé-
cules orales : dans le can-
cer colorectal métastasé et
le cancer gastrique méta-
stasé d’abord, dans le trai-
tement adjuvant du cancer
du côlon ensuite, dans les
combinaisons de radio-chi-
miothérapie ensuite.
M. Ducreux*
INTERVIEW
1
/
5
100%