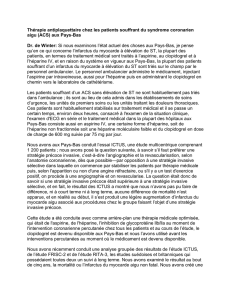
Traitement anti plaquettaire dans les SCA

Traitementantiplaquettairedans
lesSCA
Jechoisisselonlesrecommandations

Efficacitécoronaire Risquehémorragique

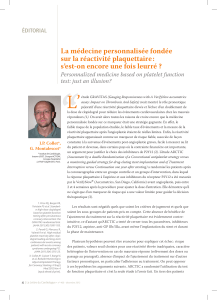
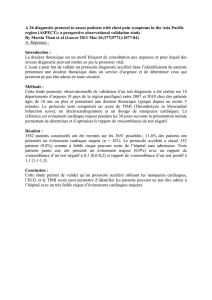
Antiplatelet Therapy in ACS
Antiplatelet Therapy in ACS
Placebo APTC CURE TRITON-TIMI 38
Single
Antiplatelet Rx Dual
Antiplatelet Rx Higher
IPA
ASA ASA +
Clopidogrel ASA +
Prasugrel
- 22%
-20%
-19%
+ 60% + 38% + 32%
Reduction
in
Ischemic
Events
Increase
in
Major
Bleeds

D’aprèsEikelboomJWetal.Circulation2006;114(8):774‐82.

Recommandations
•ESCNSTEMI2007
•ESCSTEMI2008
•ESCMyocardialrevascularisation2010
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
1
/
30
100%