Cancers différenciés de la thyroïde résistants à l`iode: quels

Cancers différenciés de la thyroïde
résistants à l’iode:
Quels traitements systémiques ?
02 décembre 2016
Dr. Olivier Mir
Département de Médecine Oncologique
Gustave Roussy, Villejuif
olivier.mir@gustaveroussy.fr

Disclosures
•Speaker for: Blueprint, Roche/Genentech, Lilly
•Consultant for: Amgen, Astra-Zeneca, Bayer, Blueprint,
Bristol Myers-Squibb, Eisai, Lilly, Novartis, Pfizer,
Roche/Genentech, Servier
•Research support (institutional) from: Astra-Zeneca,
Bayer, Blueprint, Eisai, Lilly, Novartis, PharmaMar
•Employee: Gustave Roussy

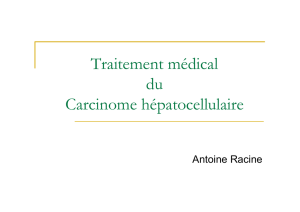
Colloide
Cellule C
Follicule
Cancer médullaire de la
thyroïde (5%)
Thyrocyte
Cancer
• Differencié (>90%)
(Papillaire, folliculaire, peu
différencié)
• Indifferencié (anaplasique)
c
Cancers de la thyroïde: classification

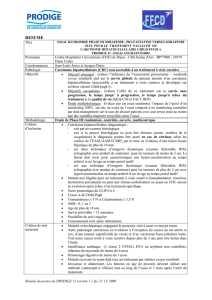
Incidence et étendue de la maladie
•Incidence des petites
tumeurs augmente.
•T3–T4: incidence stable
~10%
•Métastases à
distance:<10%.
•Cancer réfractaires
(350 cas/an en France):
•Différencié : 200 cas
•Médullaire: 50 cas
•Anaplasique: 100 cas
Sassolas et al. Eur J Endocrinol 2009;160:71
France: 7000 nouveaux cancers de la thyroïde/an, dont 4000 >1cm

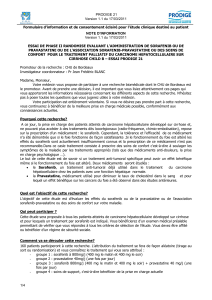
L’131I peut guérir la maladie (1/3 des patients)
Dose de radiations élevée
•Fixation de l’131I
•Dose de radiation élevée
Echec (2/3 des patients): cancers réfractaires
« Radio-sensibilité »
•Age jeune
•Tumeur bien différenciée
•Métastases petites
•Fixation du FDG absente ou
faible
•Absence de fixation au
niveau d’au moins une
lésion cible
•Progression pendant les 6-
12 mois après un traitement
par l’iode 131
•(Persistance après 22GBq)
« Radio-résistance »
•Age élevé
•Peu différencié ou bien diff.
avec mitoses ou nécrose
•Métastases volumineuses
•Fixation élevée du FDG
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
1
/
31
100%