Éléments de la personnalisation thérapeutique dans le cancer broncho-pulmonaire avancé :

382 | La Lettre du Cancérologue • Vol. XX - n° 6 - juin 2011
DOSSIER THÉMATIQUE
Cancers du poumon
Éléments de la personnalisation
thérapeutique dans le cancer
broncho-pulmonaire avancé :
de l’histologie à la biologie
moléculaire
Customized treatment in advanced lung cancer:
impact of histology and molecular biology
L. Bigay-Game*, J. Mazières*
* Service de pneumologie, clinique
des voies respiratoires, hôpital Larrey,
CHU de Toulouse ; Inserm U563,
université de Toulouse-III (Paul-
Sabatier).
L
e traitement du cancer bronchique non à
petites cellules (CBNPC) se trouve, en 2011, à
un moment charnière. D’un traitement standar-
disé au début des années 2000, comportant un des
quatre doublets associant sel de platine et molécule
de troisième génération – globalement équivalents,
en termes de résultats, à une médiane de survie
aux alentours de 8 mois –, on s’oriente progressive-
ment vers un traitement de plus en plus personna-
lisé, essentiellement basé sur le type histologique
et les biomarqueurs biologiques. Ces traitements,
administrés à des patients sélectionnés, sont asso-
ciés à des taux de réponse bien supérieurs et, dans
une moindre mesure, à des bénéfices en termes de
survie globale (SG). L’enthousiasme qui accompagne
le développement de ces nouvelles molécules ne
doit pas dispenser d’une analyse rigoureuse des
données. Nous rapportons ici les principales données
en rapport avec la personnalisation du traitement
du cancer bronchique.
Personnalisation
sur l’anatomopathologie
Antiangiogénique et type histologique
Ces dernières années, le bévacizumab, anticorps
monoclonal dirigé contre le facteur de croissance
de l’endothélium vasculaire (Vascular Endothelial
Growth Factor [VEGF]), est apparu comme une
nouvelle arme thérapeutique en première ligne
métastatique dans les CBNPC non épidermoïdes,
en association avec une bithérapie à base de sels
de platine.
Dans l’essai initial de phase II, le bévacizumab a été
évalué chez 99 patients, tous types histologiques
confondus. Suite à la survenue de 4 hémoptysies
fatales chez des patients présentant une histologie
épidermoïde associée à une tumeur proximale, le
développement du bévacizumab s’est limité aux
CBNPC non épidermoïdes (1). Plus récemment,
dans l’essai BRIDGE, étude de phase II à un bras,
J.D. Hainsworth et al. ont cherché à évaluer si l’asso-
ciation retardée (au troisième cycle) du bévacizumab
avec une chimiothérapie par carboplatine + pacli-
taxel chez des patients présentant une histologie
épidermoïde, mais sans facteurs de risque hémor-
ragique à l’inclusion, pouvait réduire le risque de
survenue d’accidents hémorragiques pulmonaires.
Un patient a eu un accident hémorragique de grade
supérieur ou égal à 3. Compte tenu du faible nombre
de patients inclus, les auteurs ont conclu que l’utili-
sation du bévacizumab dans les CBNPC épidermoïdes
ne pouvait être envisagée que dans le cadre de la
recherche clinique (2).
Les études randomisées de phase III ECOG 4599
(Eastern Cooperative Oncology Group) et AVAiL

La Lettre du Cancérologue • Vol. XX - n° 6 - juin 2011 | 383
Points forts
»
Il n’existe pas “le” cancer bronchique mais bien “des” cancers bronchiques avec des sous-groupes
histologiques et moléculaires ayant une signification pronostique et prédictive.
»
Les dernières autorisations de mise sur le marché de traitements antitumoraux en oncologie thoracique
sont conditionnées par le type histologique ou la présence d’anomalies moléculaires.
»
Des résultats très prometteurs sont enregistrés chez certains patients porteurs d’une anomalie génétique
(mutations de l’EGFR, translocation de ALK pour les plus connues) et bénéficiant de thérapies ciblant ces
anomalies.
»
Au-delà de l’enthousiasme accompagnant ces résultats, l’évaluation du bénéfice par une recherche
clinique adaptée est indispensable.
»
Les nouveaux algorithmes décisionnels en oncologie thoracique doivent désormais intégrer ces éléments
(type anatomopathologique, anomalies moléculaires) afin d’optimiser la prise en charge.
Mots-clés
Cancer bronchique
Thérapie ciblée
Anatomopathologie
EGFR
EML4-ALK
Highlights
»
Non-small-cell lung cancer
(NSCLC) is a heterogeneous
disease.
»
The most significant devel-
opment in recent years was
the discovery of activated EGFR
mutations and ALK transloca-
tion.
»
Personalized therapy
improve treatment outcomes
by identification of a specific
genotypic anomaly and target-
specific therapy.
»
Pathological subtype and
biomarkers should now be inte-
grated in decision-making and
management of lung cancer.
Keywords
Lung cancer
Targeted therapy
Anatomopathology
EGFR
EML4-ALK
(Avastin® in lung cancer), portant sur une cohorte
de CBNPC non épidermoïdes, ont montré que le
bévacizumab associé à une bithérapie apportait
un bénéfice significatif en termes de SG pour le
premier (3) et de survie sans progression (SSP)
pour le second (4) comparativement au bras stan-
dard. Une méta-analyse récente a été rapportée à
l’ESMO en 2010 et a permis d’éclaircir la place à
faire au bévacizumab dans l’arsenal thérapeutique
de première ligne. Regroupant 2 194 patients, elle
a montré un bénéfice significatif en termes de SG
et de SSP quand le bévacizumab était associé à
une bithérapie à base de platine. Il n’a pas été
montré de supériorité d’une posologie sur l’autre
(7,5 versus 15 mg/kg). Le risque de progression a
été réduit de 28 % et le risque de décès de 10 %.
L’analyse des toxicités a montré que le bévaci-
zumab augmentait significativement le risque de
survenue d’une protéinurie, d’une hypertension
artérielle, d’accidents hémorragiques et d’une
neutropénie fébrile.
Qu’en est-il de l’efficacité du bévacizumab associé
à la chimiothérapie en fonction de l’histologie dans
les CBNPC non épidermoïdes ? Les données de la
cohorte ARIES, rapportées à l’ESMO en 2010 par
J. Brahmer et al. (5), ont montré que les résultats
en termes de SSP et de SG étaient comparables.
En effet, la SSP et la SG étaient respectivement
de 6,8 et 13,7 mois pour les adénocarcinomes
(n = 1 361), de 6,3 et 12 mois pour les carcinomes
indifférenciés (n = 391) et de 6,1 et 11,2 mois pour
les carcinomes à grandes cellules (n = 87).
Certains antiangiogéniques oraux ayant pour point
commun l’inhibition de l’activité tyrosine kinase
(ITK) du VEGFR, deux d’entre eux, dont le sorafénib,
ont été évalués dans les différents types histo-
logiques de CBNPC. L’étude ESCAPE a comparé
l’efficacité d’une bithérapie par carboplatine +
paclitaxel associée ou non au sorafénib (6). Dans
le sous-groupe des patients atteints de CBNPC
épidermoïdes recevant le sorafénib, la SG était
inférieure à celle du groupe traité par bithérapie
seule, alors que, dans le groupe des CBNPC non
épidermoïdes recevant du sorafénib, il n’y avait pas
de différence en termes de SG ou de SSP. Devant
ces résultats, le sous-groupe des CBNPC épider-
moïdes initialement inclus dans l’étude NEXUS
a été retiré. Cette étude évaluait une bithérapie
par cisplatine + gemcitabine avec ou sans sora-
fénib chez 722 patients présentant un CBNPC de
stades IIIB et IV. Dans le groupe traité par sorafénib,
il n’a pas été observé d’amélioration de la SG, mais
U. Gatzemeier et al. (7) ont conclu à une amélio-
ration de la SSP et du temps jusqu’à progression.
Actuellement, le bévacizumab reste le seul anti-
angiogénique ayant l’autorisation de mise sur le
marché en première ligne métastatique dans le
CBNPC, avec une prescription exclusivement guidée
par l’anatomopathologie et réservée aux CBNPC
non épidermoïdes. Nous ne disposons pas, pour le
moment, de marqueurs cliniques ou biologiques qui
pourraient nous permettre de mieux identifier les
patients potentiellement répondeurs.
Pémétrexed et type histologique
Les premières données concernant l’“histo-
guidage” de la chimiothérapie ont été apportées
par G.V. Scagliotti et al. avec les résultats d’une
étude de phase III randomisée, de non-infériorité,
menée chez 1 725 patients présentant un CBNPC
de stade IIIB ou IV, où il a été montré un bénéfice
statistiquement significatif en termes de SG chez
les patients présentant un adénocarcinome ou un
carcinome à grandes cellules, traités par cispla-
tine + pémétrexed versus cisplatine + gemcitabine
(n = 847 ; 12,6 versus 10,9 mois) [8]. Ce résultat
mérite d’être analysé avec prudence, car il s’agit
d’une analyse de sous-groupe sans ajustement de
la valeur p pour les analyses multiples. L’histologie
comme facteur prédictif de l’efficacité du pémé-
trexed dans les CBNPC non épidermoïdes a égale-
ment été démontrée dans son indication en seconde
ligne (versus docétaxel) ainsi qu’en traitement de
maintenance (versus placebo), que ce soit en termes
de SG ou de SSG (9).
Une des raisons de la moindre efficacité du pémé-
trexed dans les CBNPC épidermoïdes pourrait être
l’existence d’une forte expression dans ces tumeurs
de la thymidylate synthase, enzyme cible de cette
molécule (9). Cependant, nous ne disposons actuel-
lement pas d’une technique fiable et reproductible
permettant de l’utiliser en routine.

384 | La Lettre du Cancérologue • Vol. XX - n° 6 - juin 2011
Éléments de la personnalisation thérapeutique dans le cancer
broncho-pulmonaire avancé : de l’histologie à la biologie moléculaire
DOSSIER THÉMATIQUE
Cancers du poumon
Cas particulier
des cancers épidermoïdes
Alors que les adénocarcinomes font l’objet de
multiples recherches et publications en termes de
traitements ciblés, les carcinomes épidermoïdes
manquent encore cruellement de cibles thérapeu-
tiques, bien que l’inhibition de certaines voies telles
que celles de l’IGF-1R (Insulin-like Growth Factor
type 1 Receptor) et du FGFR1 (Fibroblast Growth
Factor Receptor) soit en cours d’évaluation. Les
résultats concernant les anti-IGF-1R, prometteurs
en phase II, se sont néanmoins révélés décevants
en phase III.
Cas particulier
du carcinome bronchiolo-alvéolaire
La classification OMS des adénocarcinomes bron-
chiques a fait l’objet, début 2011, d’une révision
modifiant la définition du carcinome bronchiolo-
alvéolaire (CBA). Toutefois, la distinction entre les
types mucineux, non mucineux ou mixte (muci-
neux et non mucineux) persiste. Les formes muci-
neuses sont plus fréquemment observées chez les
non-fumeurs, n’expriment le plus souvent pas le
facteur de transcription thyroïdienne (TTF1) et ne
présentent pas de mutation du récepteur au facteur
de croissance épidermique (Epidermal Growth Factor
Receptor [EGFR]), mais pourraient montrer une
expression préférentielle de l’IGFR et une fréquence
élevée de mutations de l’oncogène KRAS, y compris
chez les non-fumeurs. Les formes non mucineuses
expriment, elles, le plus souvent le TTF1 et sont
fréquemment mutées pour l’EGFR. Ces caractéris-
tiques ont conduit, pour les formes étendues de CBA,
à évaluer des traitements reposant sur la chimiothé-
rapie et les ITK de l’EGFR. L’étude de phase II menée
par l’Intergroupe français de pneumo-cancérologie
(IFCT 04-01) a évalué l’efficacité et la tolérance d’un
traitement par géfitinib (250 mg/j) chez 88 patients
chimio-naïfs présentant une forme diffuse de CBA.
J. Cadranel et al. ont conclu à une différence en
termes de SG et de SSP (11,3 versus 2,6 mois) dans
les formes non mucineuses comparativement aux
formes mucineuses, sans qu’il soit possible de dire si
elle est due au pronostic différent des deux patholo-
gies ou liée à l’activité différentielle du géfitinib (10).
La chimiothérapie, et notamment le paclitaxel, a
également fait l’objet d’études de phase II, avec
une tolérance acceptable et une SSP de respecti-
vement 5,0 et 2,2 mois dans les formes mucineuses
et non mucineuses (11, 12). Le type non mucineux
constitue donc un facteur prédictif et pronostique
de meilleure réponse ou d’augmentation de la SSP
chez les patients traités par ITK de l’EGFR.
Personnalisation
sur la biologie moléculaire
L’oncogenèse du cancer bronchique est de mieux en
mieux connue. On retiendra des derniers travaux
l’importance du phénomène d’addiction onco-
génique. On retrouve deux grands types d’ano-
malies moléculaires dans les tumeurs : les mutations
motrices, à opposer aux mutations passagères. Le
terme “moteur” implique qu’elles sont essentielles
pour le maintien du phénotype tumoral. En consé-
quence, le ciblage de ces mutations devrait être plus
efficace (tableau I).
La voie de l’EGFR
Parmi les différents marqueurs biologiques actuel-
lement à notre disposition, l’EGFR est sans doute
le plus étudié. La voie de signalisation du récepteur
de l’EGF est fréquemment activée dans les cancers
bronchiques et contrôle les mécanismes d’apop-
tose, de prolifération cellulaire, de transformation et
d’angiogenèse, ce qui en fait une cible thérapeutique
de choix. Des petites molécules inhibitrices de la
fonction ITK de l’EGFR ont ainsi été développées.
Parmi elles, le géfitinib et l’erlotinib ont montré leur
intérêt chez les patients métastatiques mutés pour
Tableau I. Cibles moléculaires du cancer bronchique.
Oncogenèse Addiction oncogénique Mécanisme inconnu
Approuvé Mutation de l’EGFR
(erlotinib, géfitinib)
Angiogenèse (bévacizumab)
En cours d’exploration Translocation de ALK
Mutation de HER2
Mutation de BRAF
Activation de PI3K-AKT
Mutation de C-Kit
Mutation de FGF-R μ
Mutation de HGF
Anti-IGF-1R
Proapoptotiques
Cétuximab
Inhibiteurs de transduction du signal
Inhibiteurs du protéasome
Commentaires Événements rares
Fort taux de réponse attendu
Développement de résistances
Événements plus fréquents
Bénéfices plus faibles
Association avec une chimiothérapie
ou d’autres agents

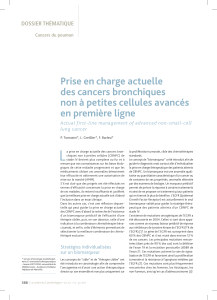
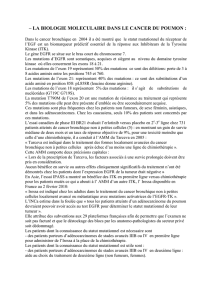
Mutations KRAS
Mutations EGFR
Mutations PI3KCA
Mutations HER2 exon 20
Mutations BRAF
Translocation EML4-ALK
Non déterminé à ce jour
3 %
3 %
3 %
2 %
57 % 12 %
20 %
Figure 1. Classification moléculaire des cancers bronchiques (source : INCA, rapport
biomarqueurs, 2010).
La Lettre du Cancérologue • Vol. XX - n° 6 - juin 2011 | 385
DOSSIER THÉMATIQUE
l’EGFR en première ligne et, quel que soit le statut
mutationnel, en deuxième ou troisième ligne (13).
On connaît, depuis 2004, l’importance des muta-
tions se produisant dans la partie du gène codant
pour le domaine tyrosine kinase du récepteur, dont
la présence est associée à une meilleure réponse
aux ITK. Des essais cliniques ont récemment validé
l’intérêt d’utiliser les ITK en première ligne thérapeu-
tique chez les patients porteurs de ces mutations.
R. Rosell et al. ont rapporté un taux de réponse
de 70,6 %, un taux de contrôle de la maladie de
89,8 %, une SSP de 14 mois et une SG de 27 mois
chez des patients mutés traités par erlotinib (14).
T.S. Mok et al. ont rapporté un bénéfice en termes de
SSP du géfitinib comparativement à une bichimio-
thérapie (13). Ce bénéfice concerne exclusivement
les patients porteurs de mutations de l’EGFR.
T. Mitsudomi et al. (15) et M. Maemondo et al. (16)
ont également rapporté très récemment la supério-
rité du géfitinib en comparaison à une chimiothérapie
chez les patients mutés. Les premiers rapportent une
SSP de 9,2 versus 6,3 mois chez les patients traités
par cisplatine et docétaxel ; les seconds rapportent
une SSP de 10,8 versus 5,4 mois chez les patients
traités par carboplatine et paclitaxel. Néanmoins,
le bénéfice, majeur en termes de SSP, peine à se
retrouver en termes de SG. Cela est probablement
dû à des effectifs insuffisants et à l’utilisation des
ITK dans des lignes ultérieures de traitement chez
les patients initialement traités par chimio thérapie.
Néanmoins, un certain nombre de patients sont
résistants aux ITK de l’EGFR malgré la présence de
mutations activatrices, et la totalité des patients
traités par ces molécules développe une résistance
secondaire dans des délais variables.
La voie EML4-ALK
Une autre voie associée à une anomalie molécu-
laire motrice a été récemment mise en évidence : il
s’agit de la translocation EML4-ALK. Des inversions
chromosomiques se produisent dans 4 à 5 % des
cancers bronchiques et aboutissent à la formation
d’un gène de fusion entre le domaine actif de la
kinase ALK1 et EML4, ce qui entraîne une activation
constitutionnelle de la kinase ALK, dont le rôle sur la
prolifération cellulaire et l’inhibition de l’apoptose
est bien connu. Cette anomalie est le plus souvent
rapportée dans les adénocarcinomes bronchiques,
chez des patients non fumeurs ou anciens fumeurs.
L’intérêt d’un inhibiteur de c-Met, le crizotinib, qui
s’est ensuite révélé être un inhibiteur puissant de
ALK-EML4, a été récemment rapporté (17). Ces résul-
tats sont tellement impressionnants qu’un essai
de phase III vient de débuter sans qu’une phase II
ait été réalisée. Très récemment, des mutations du
gène codant pour ALK ont été mises en évidence, et
sont associées à une résistance au crizotinib (18).
Tableau II. Autorisation de mise sur le marché (AMM) des différentes molécules selon l’histo-
logie et les biomarqueurs.
Molécule AMM
large
AMM/
anapath
AM/
biologie
Remarques
Sel de platine
Vinorelbine
Paclitaxel Intérêt de l’association carboplatine-paclitaxel
dans les CBA
Docétaxel
Gemcitabine Supériorité de l’association CDDP-GMZ
dans l’essai Scagliotti dans les carcinomes
épidermoïdes
Pémétrexed AMM : carcinome non épidermoïde en première
et en deuxième ligne etmaintenance
Bévacizumab AMM : non épidermoïde en première ligne
en association avec un sel de platine
Erlotinib Pas de restriction en deuxième ou en troisième
ligne. Réservé aux EGFR muté en première
ligne (AMM à venir)
Géfitinib Réservé aux EGFR muté en première ligne
Crizotinib Réservé aux translocations EML4-ALK
en première, deuxième ou en troisième ligne.
Pas d’AMM. Sur ATU
À venir Les nouvelles AMM seront conditionnées
par l’identification de cibles moléculaires
AMM : autorisation de mise sur le marché ; ATU : autorisation temporaire d’utilisation ; CBA : carcinome bronchiolo-
alvéolaire ; CDDP : cisplatine ; GMZ : Gemzar ®.

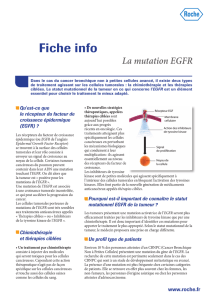
Figure 2. Schéma de la personnalisation du traitement du cancer bronchique.
Traitement
pour tous
Clinique : PS, âge, sexe, etc.
2000 2010 2020 (?)
Anatomopathologie : adénocarcinome, carcinome épidermoïde
Marqueurs biologiques : EGFR, KRAS, ALK, etc.
Micropuces ARNm, ARNmi, etc.
Protéomique, etc.
Traitement
personnalisé
Éléments de la personnalisation thérapeutique dans le cancer
broncho-pulmonaire avancé : de l’histologie à la biologie moléculaire
DOSSIER THÉMATIQUE
Cancers du poumon
1. Johnson DH, Fehrenbacher L, Novotny WF et al. Rando-
mized phase II trial comparing bevacizumab plus carbo-
platin and paclitaxel with carboplatin and paclitaxel alone
in previously untreated locally advanced or metastatic non-
small-cell lung cancer. J Clin Oncol 2004;22(11):2184-91.
2. Hainsworth JD, Fang L, Huang JE et al. BRIDGE: an open-
label phase II trial evaluating the safety of bevacizumab +
carboplatin/paclitaxel as first-line treatment for patients
with advanced, previously untreated, squamous non-small-
cell lung cancer. J Thorac Oncol 2011;6(1):109-14.
3. Sandler A, Gray R, Perry MC et al. Paclitaxel-carboplatin
alone or with bevacizumab for non-small-cell lung cancer.
N Engl J Med 2006;355(24):2542-50.
4. Reck M, von Pawel J, Zatloukal P et al. Phase III trial of
cisplatin plus gemcitabine with either placebo or bevaci-
zumab as first-line therapy for nonsquamous non-small-
cell lung cancer: AVAil. J Clin Oncol 2009;27(8):1227-34.
5. Brahmer J, Spigel D, Garst JL et al. The impact of tumor
histology on effectiveness in bevacizumab treated patients
with advanced non-small-cell lung cancer: result from ARIES,
a bevacizumab observational cohort study. Ann Oncol 2010;
21(Suppl.8).
6. Scagliotti G, Novello S, von Pawel J et al. Phase III study
of carboplatin and paclitaxel alone or with sorafenib in
advanced non-small-cell lung cancer. J Clin Oncol 2010;
28(11):1835-42.
7. Gatzemeier U, Elsen T, Santoro A. Sorafenib + gemci-
tabine/cisplatine versus gemcitabine/cisplatine alone
in the first-line treatment of advanced non-small-cell
lung cancer (NSCLC): phase III NSCLC research expe-
rience utilizing sorafenib (NEXUS) trial. Ann Oncol 2010;
21(Suppl.8).
8. Scagliotti GV, Parikh P, von Pawel J et al. Phase III
study comparing cisplatin plus gemcitabine with cisplatin
plus pemetrexed in chemotherapy-naive patients with
advanced-stage non-small-cell lung cancer. J Clin Oncol
2008;26(21):3543-51.
9. Scagliotti G, Brodowicz T, Shepherd FA et al. Treat-
ment-by-histology interaction analyses in three phase III
trials show superiority of pemetrexed in nonsquamous
non-small-cell lung cancer. J Thorac Oncol 2011;6(1):
64-70.
10. Cadranel J, Garfield D, Lavolé A, Wislez M, Milleron
B, Mayaud C. Lung cancer in HIV infected patients: facts,
questions and challenges. Thorax 2006;61(11):1000-8.
11. Scagliotti GV, Smit E, Bosquee L et al. A phase II study
of paclitaxel in advanced bronchioloalveolar carcinoma
(EORTC trial 08956). Lung Cancer 2005;50(1):91-6.
12. West HL, Crowley JJ, Vance RB et al. Advanced bron-
chioloalveolar carcinoma: a phase II trial of paclitaxel by
96-hour infusion (SWOG 9714): a Southwest Oncology
Group study. Ann Oncol 2005;16(7):1076-80.
13. Mok TS, Wu YL, Thongprasert S et al. Gefitinib or carbo-
platin-paclitaxel in pulmonary adenocarcinoma. N Engl J
Med 2009;361(10):947-57.
14. Rosell R, Moran T, Queralt C et al. Screening for
epidermal growth factor receptor mutations in lung cancer.
N Engl J Med 2009;361(10):958-67.
15. Mitsudomi T, Morita S, Yatabe Y et al. Gefitinib versus
cisplatin plus docetaxel in patients with non-small-cell lung
cancer harbouring mutations of the epidermal growth factor
receptor (WJTOG3405): an open label, randomised phase 3
trial. Lancet Oncol 2010;11(2):121-8.
16. Maemondo M, Inoue A, Kobayashi K et al. Gefitinib or
chemotherapy for non-small-cell lung cancer with mutated
EGFR. N Engl J Med 2010;362(25):2380-8.
17. Kwak EL, Bang YJ, Camidge DR et al. Anaplastic
lymphoma kinase inhibition in non-small-cell lung cancer.
N Engl J Med 2010;363(18):1693-703.
18. Choi YL, Soda M, Yamashita Y et al. EML4-ALK mutations
in lung cancer that confer resistance to ALK inhibitors. N Engl
J Med 2010;363(18):1734-9.
Références bibliographiques
Les autres voies
de signalisation motrices
Au-delà des 2 voies précédemment détaillées de
l’EGFR et de ALK, d’autres anomalies moléculaires
sont probablement à l’origine de mécanismes
d’addiction oncogénique et constituent des cibles
idéales pour une inhibition spécifique. On citera les
mutations de l’HGF, de HER2, de BRAF, de c-Kit et
d’IGF-1R (tableau I p. 384, figure 1 p. 385).
Conclusion
On démembre désormais le vaste groupe des
cancers bronchiques en sous-groupes selon le type
anatomopathologique et la présence d’anomalies
moléculaires. Au-delà de l’aspect nosographique,
ces données permettent le développement de
molécules ciblées dont certaines ont fait récem-
ment la preuve de leur efficacité (tableau II p. 385,
figure 2). L’avenir des traitements biologiques passe
par la poursuite concomitante de l’identification
de nouvelles cibles biologiques, par l’élaboration
d’inhibiteurs spécifiques et par leur validation par
une recherche clinique adaptée. ■
3e Journée européenne de la sclérodermie
29 juin 2011
Cette journée, organisée à l’initiative et avec le soutien de la
FESCA (Fédération européenne des associations de patients
sclérodermiques : 16 pays membres à ce jour) a pour objectif
d’informer les malades et le grand public sur la maladie.
Diverses manifestations, dont une conférence au Palais du
Luxembourg à Paris le 29 juin de 14 à 18 h, sont organisées en
Europe et dans toutes les grandes villes de France.
Grâce au soutien financier de l’Association des sclérodermiques
de France (ASF), 80 protocoles de recherche ont été financés
depuis 2000 pour plus d’un million d’euros. Tous les ans, l’ASF
lance un appel à projet de recherche afin de sélectionner des
protocoles de recherche à financer (dossier téléchargeable sur
le site).
Renseignements : www.association-sclerodermie.fr
Agenda
1
/
5
100%