Comment prédire la réponse à l`immunothérapie

Comment prédire la réponse à l’immunothérapie ?
Julien Adam, MD PhD
Département de Biologie et Pathologie Médicales
INSERM U981
Gustave Roussy, Villejuif

Schalper and Herbst CCR 2016


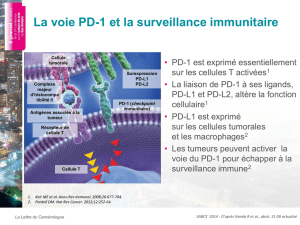
•Biomarqueur développé en
combinaison aux anti-PD1/PDL1
–Validation dans les essais de phase III
–Sélection des patients en première
ligne ou pour les combinaisons
•Valeur pronostique limitée
•Disponibilité universelle de l’IHC
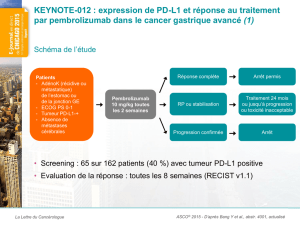
Expression de PD-L1 comme biomarqueur prédictif

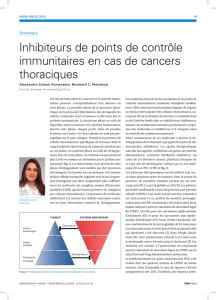
PD-L1 IHC assays
Drug Clone Epitope Detection Thresholds FDA status
Nivolumab
(BMS) 28-8
Dako Extracellular EnVision FLEX CT : ≥1%, ≥5%, ≥10% Complementary
diagnostic
(lung, melanoma)
Pembrolizumab
(MSD) 22C3
Dako Extracellular EnVision FLEX CT : ≥1%, ≥50% Companion diagnostic
(lung)
Atezolizumab
(Roche) SP142
Ventana Intracellular OptiView +
amplification CT : ≥1%, ≥5%, ≥50%
CI : ≥1%, ≥5%, ≥10%
Complementary
diagnostic (bladder)
Durvalumab
(AstraZeneca)SP263
Ventana Intracellular OptiView CT : ≥25% -
28-8 22C3 SP142 SP263
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
1
/
36
100%