Tolérance

Immunosuppression Tolerance Immunitaire
•Inhibition de toute
réponse immunitaire, non
specifique d’antigène
•Traitement chronique
•Surimmunosuppression
(incidence augmentée
d’infections, de tumeurs)
•Non réponse spécifique
de l’antigène
•Traitement court
•Effet à long terme

La Tolérance Immunitaire
Chez l’individu normal le système
immunitaire ne réagit pas de manière
agressive vis-à-vis des cellules de
l’hôte qui l’héberge

Les mécanismes de la tolérance
immunitaire
La tolérance centrale
La tolérance périphérique

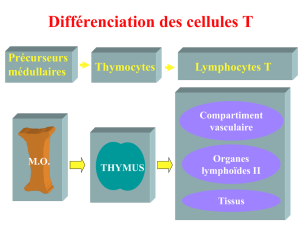
La tolérance centrale
Délétion des cellules lymphocytaires
au cours de leur différentiation
- dans le thymus (Ly T)
- dans la moelle osseuse (Ly B)
Mécanisme : apoptose

Figure 7-8
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
1
/
43
100%