Nouvelles thérapeutiques ciblant le récepteur HER2 New anti

556 | La Lettre du Cancérologue • Vol. XIX - n° 9 - novembre 2010
MISE AU POINT
Nouvelles thérapeutiques
ciblant le récepteur HER2
New anti-HER2 therapeutic strategies
V. Diéras*
* Institut Curie, Paris.
Le récepteur de facteur de croissance HER2 est
un facteur pronostique et prédictif important
dans les cancers du sein, que ce soit en
situation adjuvante ou métastatique. Le gène
HER2 est amplifié et la protéine HER2 surexprimée
dans 15 à 20 % des cas. Également connu sous le
nom de HER2/neu ou c-erbB2, il est localisé sur le
chromosome 17q et appartient à la famille des gènes
de récepteurs de facteurs de croissance HER. Il code
pour une protéine transmembranaire de 185 kDa,
récepteur de facteurs de croissance avec activité
tyrosine kinase, entraînant la signalisation pour la
prolifération et la survie cellulaires.
Le trastuzumab, un anticorps monoclonal humanisé
se fixant sur le récepteur, a démontré son effi-
cacité dans les cancers du sein aux stades précoce
et métastatique (1). Cependant, s’il représente
la clé de voûte des traitements du cancer du sein
surexprimant HER2, il existe des résistances. En
situation métastatique, elles sont fréquentes :
60 à 70 % en monothérapie, 30 % en association
avec la chimiothérapie. À un moment donné,
tous les cancers du sein métastatiques présentent
une progression sous trastuzumab. En situation
adjuvante, après traitement par trastuzumab, des
récidives surviennent également.
La surexpression de HER2 ne suffit pas à assurer
une sensibilité au trastuzumab ; d’autres voies de
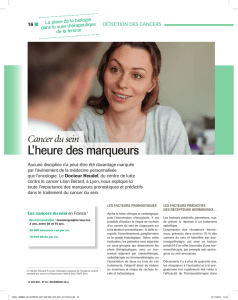
signalisation sont impliquées. Différents mécanismes
sont évoqués et présentés sur la figure 1 : activation
de la voie de signalisation IGF-1, récepteur tronqué,
activation HER3, activation de la voie PI3K (2).
Il existe donc un besoin réel de développer de
nouvelles thérapeutiques ciblées (3).
Ce développement repose en grande partie sur les
hypothèses biologiques de résistance au trastuzumab
(figure 1). Schématiquement, ces nouvelles théra-
peutiques comprennent les petites molécules ciblant
le site tyrosine kinase du récepteur, de nouveaux
anticorps, les inhibiteurs du signal de transduction
et les inhibiteurs d’HSP90 (figure 2).
Les inhibiteurs de tyrosine
kinase
Ces petites molécules, administrées par voie
orale, agissent au niveau du site tyrosine kinase du
récepteur HER2. Elles inhibent également, à un degré
variable, les tyrosine kinases des autres récepteurs
(HER1, HER4). Les inhibiteurs de tyrosine kinase
agissent par compétition avec l’adénosine triphos-
phate (ATP) au niveau de la portion intracellulaire
du récepteur. Le rationnel de développement de
ces molécules repose sur 2 grands principes : le
ciblage du récepteur tronqué HER2 et l’inhibition
de plusieurs récepteurs de la famille HER.
Dans 25 % des tumeurs surexprimant HER2, un
processus protéolytique aboutit à un récepteur
tronqué (p95 – HER2), qui présente une activité
tyrosine kinase augmentée. L’expression de ce
récepteur est corrélée à un mauvais pronostic
et à une résistance au trastuzumab (2). L’inhi-
bition de plusieurs récepteurs peut contourner le
mécanisme de résistance dû à l’activation colla-
térale des autres protéines de la famille HER. Le
passage de ces molécules au niveau de la barrière
hémato-méningée et leur activité sur les métastases
cérébrales, fréquentes dans les cancers du sein surex-
primant HER2, sont d’autres intérêts potentiels de
leur développement.
Lapatinib
Le lapatinib, un inhibiteur réversible de tyrosine
kinase ciblant HER1 et HER2, est actuellement le
seul enregistré après progression sous trastuzumab.

Mutations de PI3K
Activation d’AKT
PTEN
(délétion ou mutation)
HER2 tronquée
Surexpression du ligand
Dégradation
de p27
HER1-HER1
HER1- HER3+++
Apoptose
cdk2 p27 Cycline
p
MEK 1/2
GRP SOS
RAS
RAF
p85
p110
src
PTEN
PI3 kinase
IRS1
Tyrosine
kinase IGF1 signalling
Famille HER
ERBB2
AKT
src
p27
p27
MAP kinase
p27
dégradation
Prolifération Angiogenèse
Noyau
Cytoplasme
Interaction IGF1-R/HER2
Figure 1. Mécanismes de résistance au trastuzumab.
Apoptose
cdk2 p27 Cycline
p
MEK 1/2
GRP SOS
RAS
RAF
p85
p110
src
PTEN
PI3 kinase
IRS1
Tyrosine
kinase IGF1 signalling
Famille HER
erbB2
AKT
src
p27
p27
MAP kinase
p27
dégradation
Prolifération Angiogenèse
Noyau
Cytoplasme
Inhibiteurs de PI3K
Inhibiteurs de mTOR
et AKT
Lapatinib
Nératinib
Inhibiteurs
de HSP90
T-DM1
T-DM1
Anti-IGF1-R
Pertuzumab
Inhibiteurs de HDAC
mTOR
Figure 2. Nouveaux ciblages thérapeutiques anti-HER2.
La Lettre du Cancérologue • Vol. XIX - n° 9 - novembre 2010 | 557
Résumé
Le trastuzumab, anticorps ciblant HER2, représente une avancée majeure dans le traitement des cancers
du sein surexprimant HER2, que ce soit au stade précoce ou en situation métastatique. Cependant, il existe
des résistances, et de nouvelles stratégies thérapeutiques sont nécessaires pour améliorer le pronostic.
Cette revue présente les nouvelles thérapeutiques émergeantes, incluant essentiellement les inhibiteurs
de tyrosine kinase, les nouveaux anticorps et les inhibiteurs de la transmission du signal.
Mots-clés
Cancer du sein
métastatique
HER2
Thérapeutiques ciblées
Anticorps
monoclonaux
Trastuzumab
Pertuzumab
Lapatinib
Neratinib
T-DM1
Highlights
Trastuzumab, monoclonal anti-
body targeting HER2, marked a
breakthrough in the treatment
of HER2 positive breast cancer
patients with a large effect in
early and advanced stages of
the disease. However, resis-
tances occur and new thera-
peutic strategies are needed in
order to improve the outcome.
This review presents emerging
therapeutic approaches
including mainly tyrosine
kinase inhibitors, novel mono-
clonal antibodies, and signal
transduction inhibitors.
Keywords
Metastatic breast cancer
HER2
Targeted therapies
Monoclonal antibodies
Trastuzumab
Pertuzumab
Lapatinib
Neratinib
T-DM1

Figure 3. Sites de
liaison des anticorps
sur le récepteur HER2.
Pertuzumab/trastuzumab
Pertuzumab
Trastuzumab
Extracellulaire
Intracellulaire
Domaine
tyrosine
kinase
ErbB2
HER2
neu
558 | La Lettre du Cancérologue • Vol. XIX - n° 9 - novembre 2010
Nouvelles thérapeutiques ciblant le récepteur HER2
MISE AU POINT
Dans les études précliniques, le lapatinib ne présente
pas de résistance croisée avec le trastuzumab.
Dans les essais de phase I, des réponses ont été
observées chez des patientes lourdement prétraitées.
Les essais de phase II ont montré que le lapatinib
présentait une activité et une tolérance acceptables.
Les principaux effets secondaires sont des rashs et
des diarrhées.
Dans l’étude pivotale d’enregistrement, chez
des patientes présentant une progression après
un traitement par anthracyclines, taxanes et
trastuzumab, l’association capécitabine et lapatinib
est supérieure à la capécitabine seule en termes de
réponse objective (RO) [27 à 48 %] et de temps jusqu’à
progression (5,6 à 8,2 mois) [4]. Un autre essai de
phase III compare, dans la même situation, le lapatinib
associé ou non à du trastuzumab : la poursuite du
trastuzumab non seulement s’accompagne d’une
augmentation de la survie sans progression mais se
traduit également par une augmentation significative
de la survie globale, ce qui montre l’intérêt potentiel
d’un blocage complet du récepteur HER2 (5). Dans
un essai de phase III comparant paclitaxel avec ou
sans lapatinib, l’apport du lapatinib apparaît dans la
population de patientes présentant une tumeur du
sein surexprimant HER2 (6). Des associations avec
d’autres cytotoxiques sont par ailleurs évaluées dans
des essais de phase I/II, importants à réaliser du fait
d’une interaction pharmacocinétique. Le lapatinib
diffuse au niveau cérébral : ainsi, dans un essai de
phase II, une activité dans les métastases cérébrales a
été objectivée (7). En situation adjuvante, le lapatinib
est en évaluation dans 2 grands essais cliniques
(TEACH [Tykerb® Evaluation After Chemotherapy]
et ALTTO [Adjuvant Lapatinib and/or Trastuzumab
Treatment Optimisation]). L’essai néo-adjuvant
NEO-ALTTO devrait permettre de préciser les facteurs
prédictifs de réponse au lapatinib et au trastuzumab.
Neratinib (HKI-272)
Le neratinib est un inhibiteur irréversible pan-HER
(HER1, HER2 et HER4). Dans les études de phase I (8),
la toxicité limitant la dose était la diarrhée. Dans une
large étude de phase II (9), une RO a été observée
chez 51 % des patientes qui n’avaient pas reçu de
trastuzumab antérieurement et chez 26 % des
patientes prétraitées par trastuzumab (3).
Les nouveaux anticorps
Pertuzumab
Le pertuzumab est un anticorps monoclonal
humanisé se fixant sur un épitope différent de celui
du trastuzumab, empêchant la dimérisation des
récepteurs (figure 3) [10]. Ainsi, il bloque la faculté
du récepteur HER2 de former des hétérodimères avec
les autres membres de la famille HER, empêchant
la transmission du signal. Les études précliniques
ont montré une synergie entre le trastuzumab et
le pertuzumab qui peut contourner le mécanisme
de résistance du trastuzumab. Dans les études de
phase I (11), le pertuzumab est bien toléré, et une
activité antitumorale a été objectivée. Les effets
secondaires les plus fréquents sont représentés
par les diarrhées, l’asthénie, les nausées-vomis-
sements et les rashs. Les résultats d’une étude de
phase II suggèrent que l’association trastuzumab
et pertuzumab entraîne un bénéfice clinique après
progression sous trastuzumab (12). Un essai de
phase III (étude CLEOPATRA [CLinical Evaluation
Of Pertuzumab And TRAstuzumab]) comparant
docétaxel-trastuzumab-pertuzumab à docétaxel-
trastuzumab-placebo en première ligne métastatique
est en cours.
Trastuzumab-DM1
L’une des stratégies pour contourner la résistance au
trastuzumab est d’augmenter l’activité de l’anticorps.
Le trastuzumab-MCC-DM1(T-DM1) associe cette
molécule à un agent cytotoxique, la maytansine,
qui est libérée dans le cytoplasme et permet ainsi
une approche cytotoxique plus ciblée, avec moins
d’effets secondaires (13). La maytansine est un
inhibiteur puissant de l’assemblage des microtu-
bules, mais son développement avait été inter-
rompu en raison d’une toxicité importante dans
les études cliniques. Le MCC est un composé qui
stabilise le lien avec le trastuzumab dans la circu-
lation générale et qui permet la libération au niveau
intracellulaire, maintenant ainsi une efficacité et
diminuant la toxicité. Dans les études de phase I
évaluant 2 schémas d’administration (administration
hebdomadaire et toutes les 3 semaines), des RO et

En direct
Avec le soutien institutionnel de
San Antonio, 9-12 décembre 2010
Annual San Antonio
Breast Cancer Symposium
33rd
Coordinateur :
Pr Jean-François Morère, Bobigny
SABCS
SABCS
SITE RÉSERVÉ AUX PROFESSIONNELS DE LA SANTÉ
Journal en ligne
les temps forts du congrès
3310EONC25 - Novembre 2010
www.edimark.fr/ejournaux/sabcs2010
Consultation sur :
“Attention : ceci est un compte-rendu de congrès dont l’objectif est de fournir des informations
sur l’état actuel de la recherche ; ainsi, les données présentées sont susceptibles de ne pas être
validées par les autorités françaises et ne doivent donc pas être mises en pratique.”
“Ces informations sont sous la seule responsabilité des auteurs et du directeur
de la publication qui sont garants de l’objectivité de cette publication.”
La Lettre du Cancérologue • Vol. XIX - n° 9 - novembre 2010 | 559
des stabilisations ont été observées (3). La toxicité
limitant l’augmentation de dose était une thrombo-
pénie de grade supérieur à 2. Il n’a pas été observé de
toxicité cardiaque. Dans 2 larges études de phase II,
le T-DM1 a été administré à la dose de 3,6 mg/kg
toutes les 3 semaines chez des patientes présentant
un cancer du sein métastatique surexprimant HER2
et progressant après traitement par trastuzumab. Les
taux de RO étaient de 32 et de 40 % (3). La throm-
bopénie et l’hypokaliémie ont été les principales
toxicités de grades 3 et 4. Les études de phase III en
première ligne ou au-delà de la première ligne sont
en cours (études MARIANNE et EMILIA).
Ertumaxomab
La résistance au trastuzumab peut également être
contournée en formulant des anticorps ayant un
double mécanisme d’action. L’ertumaxomab est un
anticorps monoclonal, bispécifi que fi xant à la fois
HER2 et CD3. Les liaisons forment un complexe de
cellules T, de cellules HER2+ et de macrophages ou
cellules dendritiques conduisant à la phagocytose des
cellules tumorales. Dans l’étude de phase I (3, 14),
une RO a été notée et les principaux effets secon-
daires étaient la fi èvre, les frissons, les céphalées
et les nausées-vomissements. Les toxicités de
grades 3 et 4 comprenaient une lymphopénie et une
cytolyse (14). Des études de phase II sont en cours.
Les inhibiteurs
de la transmission du signal
Inhibiteurs de mTOR
La perte d’activité de PTEN (Phosphatase and
TENsin homolog) a été associée à la résistance au
trastuzumab (15). Les kinases mTOR (mammalian
Target Of Rapamycin) régulent PTEN et sont des
médiateurs importants de la signalisation PI3K-AKT
(fi gure 1). Ce circuit, une fois activé, conduit à la
prolifération cellulaire et est régulé de façon négative
par PTEN. La rapamycine a été le premier inhibiteur
de mTOR, mais d’autres analogues (temsirolimus,
évérolimus et ridaforolimus) ont été développés
pour augmenter sa stabilité et sa solubilité. En
monothérapie, son activité est faible. En revanche,
en association avec la chimiothérapie (paclitaxel
ou vinorelbine) et le trastuzumab, des RO ont été
observées (3). Des études de phase III sont en cours
(dont les études BOLERO).

Nouvelles thérapeutiques ciblant le récepteur HER2
MISE AU POINT
Inhibiteurs de PI3 kinase
L’activation de la voie PI3 kinase (PI3K) est impor-
tante dans la signalisation HER2 (16). Des mutations
de PI3K ont été associées à une résistance au
trastuzumab. De nombreux inhibiteurs de PI3K sont
actuellement en développement précoce.
Les autres approches
Ciblage de la voie IGF-IR
L’activation de la voie de l’IGF-IR (Insulin-like Growth
Factor-1 Receptor) a été le premier mécanisme décrit
de résistance au trastuzumab (17). Comme pour
les récepteurs de la famille HER, le ciblage peut
s’effectuer par des anticorps ou par des molécules
inhibant le site tyrosine kinase. De nombreux
anticorps sont en voie de développement.
Agents antiangiogéniques
Il existe une corrélation entre la surexpression HER2
et l’expression du VEGF, conduisant à l’évaluation
de l’inhibition simultanée de ces deux circuits.
L’association d’agents antiangiogéniques (anticorps
comme le bévacizumab ou inhibiteur de tyrosine
kinase comme le pazopanib) aux agents ciblant HER2
a démontré une efficacité potentielle en cours de
confirmation dans les essais randomisés (3).
Inhibiteurs de HSP90
HSP 90 (Heat Shock Protein 90) est une protéine
chaperone qui stabilise des protéines telles
que HER2, AKT, EGFR (Epithelial Growth Factor
Receptor) et PDGFR (Platelet-Derived Growth
Factor Receptor). L’inhibition de HSP 90 induit
une dégradation du protéosome et une inhibition
tumorale (18). Ce mécanisme peut être utilisé
pour contrecarrer la résistance au trastuzumab.
Le développement du premier inhibiteur, la
geldanamycine, a été interrompu en raison d’une
toxicité hépatique. Dans les études précliniques,
la tanespimycine était moins toxique et induisait
une diminution d’expression de la protéine HER2
et de la croissance cellulaire. Dans les études de
phases I et II, chez des patientes présentant un
cancer du sein surexprimant HER2 et recevant du
trastuzumab hebdomadaire associé à la tanespi-
mycine, des réponses ont été observées (19). Les
principaux effets secondaires étaient des céphalées,
de l’asthénie, des diarrhées et une cytolyse
hépatique. Des inhibiteurs de HSP 90 de seconde
génération, dont l’alvespimycine sont en cours de
développement et d’évaluation (20).
Conclusion
Le pronostic des cancers du sein HER2 a été considé-
rablement amélioré par le trastuzumab. En situation
métastatique, il prolonge la survie sans progression
et la survie globale, mais une évolutivité survient
chez la majorité des patientes. Les mécanismes de
résistance sont variés, de nombreux agents sont en
cours d’évaluation dans cette situation et certains
semblent très prometteurs. À l’avenir, il est très
vraisemblable qu’il faudra envisager l’association
de plusieurs thérapeutiques ciblées afin de prévenir
la résistance. Le challenge sera alors de définir les
associations et leurs séquences optimales, fondées
sur des données biologiques. Dans cette optique,
les essais cliniques en situation préopératoire ou
néo-adjuvante représentent le meilleur modèle. ■
1. Pegram MD, Konecny G, Slamon DJ. The molecular and
cellular biology of HER2/neu gene amplification/overexpres-
sion and the clinical development of herceptin (trastuzumab)
therapy for breast cancer. Cancer Treat Res 2000;103:57-75.
2. Spector NL, Blackwell KL. Understanding the mecha-
nisms behind trastuzumab therapy for human epidermal
growth factor receptor 2-positive breast cancer. J Clin Oncol
2009;27(34):5838-47.
3. Jones KL, Buzdar AU. Evolving novel anti-HER2 strategies.
Lancet Oncol 2009;10(12):1179-87.
4. Geyer LE, Forster J, Lindquist D et al. Lapatinib plus cape-
citabine for HER2-positive advanced breast cancer. N Engl
J Med 2006;355(26):2733-43.
5. Blackwell KL, Burstein HJ, Storniolo AM et al. Randomized
study of lapatinib alone or in combination with trastuzumab
in women with ErbB2-positive, trastuzumab-refractory
metastatic breast cancer. J Clin Oncol 2010;28(7):1124-30.
6. Di Leo A, Gomez HL, Aziz Z et al. Phase III, double-blind,
randomized study comparing lapatinib plus paclitaxel with
placebo plus paclitaxel as first-line treatment for metastatic
breast cancer. J Clin Oncol 2008;26(34):5544-52.
7. Lin NU, Diéras V, Paul D et al. Multicenter phase II study
of lapatinib in patients with brain metastases from HER2-
positive breast cancer. Clin Cancer Res 2009;15(4):1452-9.
8. Wong KK, Fracasso PM, Bukowski RM et al. A phase I study
with neratinib (HKI-272), an irreversible pan-ErbB receptor
tyrosine kinase. Clin Cancer Res 2009;15(7): 2552-8.
9. Burstein HJ, Sun Y, Dirix LY et al. Neritinib, an irrever-
sible ErbB receptor tyrosine kinase inhibitor, in patients
with advanced ErbB2-positive breast cancer. J Clin Oncol
2010;28(8):1301-7.
10. Franklin MC, Carey KD, Vajdos FF et al. Insights into
ErbB signalling from the structure of the ErbB2-pertuzumab
complex. Cancer Cell 2004;5(4):317-28.
11. Agus DB, Gordon MS, Taylor C et al. Phase I clinical
study of pertuzumab, a novel HER dimerization inhi-
bitor, in patients with advanced cancer. J Clin Oncol
2005;23(11):2534-43.
12. Baselga J, Gelmon KA, Verma S et al. A phase II trial
of pertuzumab and trastuzumab in patients with human
epidermal growth factor receptor 2-positive metastatic
breast cancer that progressed during prior trastuzumab
therapy. J Clin Oncol 2010;28(7):1138-44.
13. Lewis Phillips GD, Li G, Duggert DL et al. Targeting HER2-
positive breast cancer with trastuzumab-DM1, an antibody-
cytotoxic drug conjugate. Cancer Res 2008; 68(22):9280-90.
14. Jäger M, Schoberth A, Ruf P, Hess J, Lindhofer H. The
trifunctional antibody ertumaxomab destroys tumor cells
that express low levels of human epidermal growth factor
receptor 2. Cancer Res 2009;69(10):4270-6.
15. Nagata Y, Lan KH, Zhou X et al. PTEN activation contri-
butes to tumor inhibition by trastuzumab, and loss of PTEN
predicts trastuzumab resistance in patients. Cancer Cell
2004;6(2):117-27.
16. Berns K, Horlings HM, Hennessy BT et al. A functional
genetic approach identifies the PI3K pathway as a major
determinant of trastuzumab resistance in breast cancer.
Cancer Cell 2007;12(4):395-402.
17. Courtney KD, Corcoran RB, Engelman JA. The PI3K
pathway as drug target in human cancer. J Clin Oncol
2010;28(6):1075-83.
18. Holzbeierlein JM, Windsperger A, Vielhauer G. Hsp90: a
drug target? Curr Oncol Rep 2010;12(2):95-101.
19. Nahta R, Yuan LX, Zhang B, Kobayashi R, Esteva FJ. Insulin-
like growth factor-1 receptor/human epidermal growth factor
receptor 2 heterodimerization contributes to trastuzumab resis-
tance of breast cancer cell. Cancer Res 2005;65(23):11118-28.
20. Modi S, Stopeck AT, Gordon MS et al. Combination of
trastuzumab and tanespimycin (17-AAG, KOS-953) is safe
and active in trastuzumab-refractory HER-2 overexpressing
breast cancer: a phase I dose-escalation study. J Clin Oncol
2007;25(34):5410-7.
Références bibliographiques
1
/
5
100%