Mise au point Endoprothèses coronaires et diabète

133
Métabolismes Hormones Diabètes et Nutrition (XII), n°3, mai-juin 2008
Mise au point
Mise au point
L
e nombre de sujets adultes diabétiques, en constante
augmentation, peut être estimé à plus de 150 mil-
lions de par le monde (1). La mortalité de cette
population est attribuable au moins pour moitié à une
cause cardiovasculaire, au premier rang desquelles l’in-
suffisance coronarienne (1). Les diabétiques ont deux à
quatre fois plus de risque de développer, et de développer
plus tôt, une cardiopathie ischémique que les non diabéti-
ques (2). Malgré un traitement médicamenteux optimisé,
une proportion non négligeable de ces patients, suite à
un syndrome coronarien aigu ou après dépistage systé-
matique d’une ischémie myocardique silencieuse étendue
et sévère, nécessitera un geste de revascularisation. Quel
que soit le mode de revascularisation, chirurgicale par
pontages coronariens (PC) ou par intervention coronaire
percutanée (ICP), la présence d’un diabète est associée à
un pronostic péjoratif (3, 4). L’objectif de cette revue est
de résumer, devant l’essor de cette technique, à la lumière
des spécificités liées au diabète et des preuves scientifi-
ques à notre disposition, les indications et les résultats
des ICP avec emploi d’endoprothèses coronaires chez le
diabétique.
Particularités du patient diabétique
Il s’agit de l’ensemble des facteurs liés au diabète,
influençant le développement de l’athérosclérose et de
ses complications thrombotiques, et pesant de manière
péjorative sur le pronostic de ces patients, qu’ils soient
revascularisés ou non.
On y retrouve des anomalies métaboliques et hématolo-
giques telles que l’hyperglycémie, l’insulinorésistance,
l’inflammation génératrice de dysfonction endothéliale,
l’hyperagrégabilité plaquettaire liée notamment à une
surexpression plaquettaire des récepteurs aux glycopro-
téines IIbIIIa (5, 6). Du point de vue anatomique, des
études autopsiques et angiographiques ont démontré
que les diabétiques développent plus souvent des lésions
coronaires diffuses, pluritronculaires et atteignant le
tronc commun coronaire gauche (TCG) [7-9], avec des
diamètres luminaux des lits d’aval plus faibles et davan-
tage d’occlusions chroniques (9, 10). Alors que l’on peut
assister, en réponse à une obstruction coronaire ancienne,
à la formation d’un réseau de collatérales pouvant
constituer un véritable pontage intrinsèque protégeant
le myocarde menacé, on observe chez le diabétique
une capacité moindre à développer cette collatéralité
(11). Enfin, au niveau de la structure même de la plaque
d’athérome, il existe chez les patients diabétiques plus de
plaques riches en lipides susceptibles de se rompre (12).
Endoprothèses coronaires et diabète
Nicolas Dumonteil*, Nicolas Boudou*, Michel Galinier*, Didier Carrié*
* Fédération de cardiologie, pôle cardiovasculaire et métabolique,
CHU Rangueil, Toulouse.
L’athérosclérose coronaire du patient diabétique
est le plus souvent diffuse, sévère, pluritronculaire
et/ou atteignant le tronc commun coronaire gauche
(TCG).
Le fait d’être diabétique est associé à un pronostic
péjoratif après revascularisation coronarienne, qu’elle
soit chirurgicale ou percutanée.
Le diabète est un facteur prédictif indépendant de
resténose après angioplastie coronaire.
Les endoprothèses coronaires actives ou drug
eluting stents (DES) sont constituées d’une plateforme
métallique recouverte d’un polymère qui délivre une
drogue cytotoxique inhibant la prolifération néo-inti-
male, source de resténose.
Les DES réduisent le taux de resténose par rapport
aux endoprothèses coronaires métalliques ou bare
metal stent (BMS), y compris chez le diabétique.
La chirurgie de pontages coronaires (PC) reste la
méthode de référence de revascularisation des diabé-
tiques pluritronculaires.
La revascularisation coronaire percutanée (ICP) est
indiquée chez le diabétique devant des lésions focales
mono- ou bitronculaires, avec si possible, implanta-
tion d’un DES plutôt que d’un BMS.
En cas d’ICP avec implantation d’un DES, une
double antiagrégation plaquettaire doit être prolongée
pour une durée minimale d’un an, avec poursuite d’un
seul antiagrégant à vie ensuite.
S
S
S
S
S
S
S
S
points FORTS

134
Métabolismes Hormones Diabètes et Nutrition (XII), n°3, mai-juin 2008
Mise au point
Mise au point
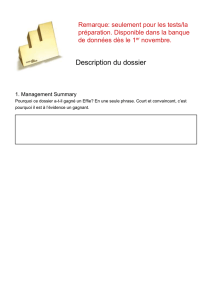
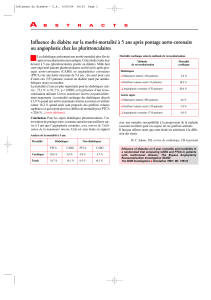
Tableau. Essais randomisés ayant comparé PC et ICP : analyse des sous-groupes de patients diabétiques (adapté de 3).
Étude Type de patients Groupes Revascularisations
répétées (%) Mortalité (%) p
BARI, 1996 Pluritronculaires PC (n = 180) 11,1% à 7 ans 19,4% à 5 ans 0,003
Ischémie prouvée ICP (n = 173) 69,9% à 7 ans 34,5% à 5 ans
PC 25,6% à 7 ans 0,001
ICP 44,3% à 7 ans
ARTS, 2001 Pluritronculaires PC (n = 96) 3,1% à 1 an 3,1% à 1 an 0,294
Ischémie prouvée ICP (n = 112) 22,3% à 1 an 6,3% à 1 an
FE VG > 30% PC 8,4% à 3 ans 4,2% à 3 ans 0,39
ICP 41,1% à 3 ans 7,1% à 3 ans
AWESOME, 2001 Patients à haut risque chirurgical PC (n = 79) 35% à 1 an 19% à 1 an 0,27
ICP (n = 65) 49% à 1 an 14% à 1 an
Angor réfractaire PC 46% à 5 ans 34% à 5 ans 0,27
ICP 51% à 5 ans 26% à 5 ans
FE VG : fraction d’éjection du ventricule gauche.
Les méthodes de revascularisation
coronaire
C’est la chirurgie de PC qui, historiquement, est la méthode
de référence. Néammoins, la nécessité d’une anesthésie
générale, d’une thoracotomie, d’une circulation extra-
corporelle – avec ses complications cérébrales potentielles
– et d’une convalescence prolongée ont fait que, bénéficiant
de progrès technologiques constants ces dernières années
et malgré des risques propres non négligeables sur lesquels
nous reviendrons, les ICP se sont imposées dans certaines
indications. Ainsi, devant une lésion focale monotron-
culaire, on comprendra aisément que la balance bénéfices/
risques penche en faveur d’une revascularisation par voie
endoluminale. De même, à la phase aiguë de constitution
d’un infarctus du myocarde avec surélévation du segment
ST durant laquelle l’urgence est à la recanalisation de
l’artère coronaire coupable occluse, les délais de mise en
œuvre d’un PC rendent cette méthode inappropriée.
Cependant, les patients diabétiques sont plus souvent
porteurs de lésions coronaires diffuses, pluritronculaires,
atteignant le TCG, pour lesquelles le choix du mode de
revascularisation n’est pas aussi clair. Il peut tout de même
être guidé par un certain nombre de preuves scientifiques.
Il n’y a pas d’essai prospectif randomisé mené exclusive-
ment au sein d’une population de diabétiques, comparant
PC et ICP en termes de mortalité, qui ait été publié à
ce jour. On dispose cependant de plusieurs essais ayant
comparé ces deux stratégies avec analyses de sous-
groupes de patients diabétiques.
Parmi les premiers ayant été conduits, l’essai BARI
(Bypass Angioplasty Revascularization Investigation)
est celui qui retient le plus l’attention (13). Y ont été
comparés PC et ICP au ballon comme modes de revas-
cularisation chez des patients pluritronculaires avec
ischémie prouvée. Dans la sous-population de diabétiques
(n = 353), on constate une réduction absolue de morta-
lité de 15,1% à 5 ans (p = 0,003) et de 18,7 % à 7 ans
(p = 0,001) en cas de PC et une nécessité plus impor-
tante de revascularisations répétées en cas d’ICP (69,9%
contre 11,1% en cas de PC à 7 ans). Au sein de la popu-
lation globale, on observe cette même différence tandis
que la mortalité, elle, ne diffère pas de manière signi-
ficative (tableau). Ces données ont un intérêt purement
historique et ne peuvent en aucun cas être extrapolées à
la pratique quotidienne car les endoprothèses coronaires
et l’environnement pharmacologique actuel encadrant les
ICP ne furent pas employées dans cet essai. Cela explique
le grand nombre de revascularisations répétées au cours
du suivi dans le bras ICP, en raison principalement de
resténoses, et permet de comprendre la généralisation de
l’emploi des endoprothèses coronaires.
Les endoprothèses coronaires métalliques
ou bare metal stents (BMS)
Les BMS ont été développés en réponse aux complications
des ICP au ballonnet telles que les dissections, occlusions
aiguës et, à plus long terme la resténose, réaction d’hy-
perplasie néo-intimale au niveau du site dilaté. L’emploi
systématique de ces endoprothèses par comparaison à une
stratégie ne les réservant qu’aux complications aiguës ou
aux résultats incomplets des ICP au ballon a permis une
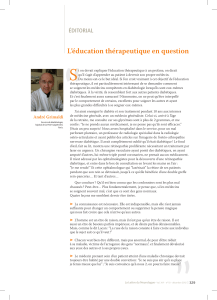
réduction du taux de resténose de 40% à 27%, sans toute-
fois qu’il y ait de bénéfice en termes de mortalité ou de
survenue d’infarctus du myocarde après la procédure (14)

135
Métabolismes Hormones Diabètes et Nutrition (XII), n°3, mai-juin 2008
Mise au point
Mise au point
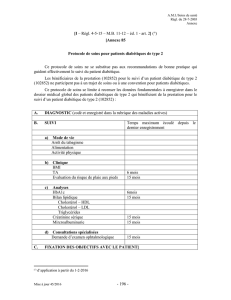
0
2
5,4
OR = 0,9
(0,72-1,11)
OR = 1,01
(0,79-1,31)
Décès et IdM
PTCA BMS
Pontage coronarien
4,8
2,8 3
4
6
8
(%)
0
10
40
OR = 0,52
(0,4-0,7)
OR = 0,59
(0,5-0,7)
Resténose ICP répétée
27
16,3
10,8
30
40
50
(%)
20
Figure 1. Méta-analyse des essais comparant ICP avec implantation systématique de BMS versus ICP au ballon + BMS uniquement si complication
aigüe (adapté de 14).
BMS : bare metal stent – PTCA : percutaneous transluminal coronary angioplasty.
[figure 1]. De nombreux facteurs prédictifs de resténose,
indépendants, ont été identifiés, au premier rang desquels
le diabète (15). Dès lors, au regard des résultats de BARI, il
était légitime de s’interroger sur les bénéfices des ICP avec
emploi de BMS par rapport à la chirurgie chez le diabé-
tique. L’étude ARTS (Arterial Revascularization Therapy
Study) a comparé PC et ICP avec implantation de BMS
chez des patients pluritronculaires avec ischémie prouvée
(16). Dans le sous-groupe de patients diabétiques (n = 208),
aucune différence statistiquement significative n’a été
observée entre les deux méthodes en termes de mortalité à
1 et 3 ans (tableau). Les patients traités par ICP ont néces-
sité plus de nouvelles procédures de revascularisation au
cours du suivi, notamment plus de PC (10% versus 2%,
p < 0,05), en raison de la resténose mais également d’un
taux de revascularisation complète obtenu par ICP plus bas
que celui obtenu par PC (70,5% versus 84,1%, p < 0,001).
Un autre essai comparatif entre PC et ICP mené chez des
patients à plus haut risque (Angina With Extremely Serious
Operative Mortality Evaluation, AWESOME) a permis de
retrouver, toujours au sein d’un sous-groupe de diabéti-
ques, des résultats comparables à ceux de ARTS pour ce
qui est de la mortalité et de la nécessité de revascularisa-
tions répétées en cas d’ICP (17) [tableau].
Ces données suggèrent donc que le principal inconvénient
de la revascularisation par ICP avec emploi de BMS par
rapport au PC chez le diabétique pluritronculaire réside
dans un risque beaucoup plus important de revascularisa-
tions répétées, elles-mêmes en grande partie secondaires à
la resténose intrastent. Il faut cependant souligner que le
faible recul vis-à-vis de ces essais ne permet pas de savoir
si, à l’échelle du suivi d’un patient dans la pratique quoti-
dienne, s’étalant sur plusieurs années, l’absence de diffé-
rence en termes de mortalité entre ICP et PC se maintient.
Les endoprothèses coronaires actives
ou drug eluting stents (DES)
Il s’agit de la solution technologique proposée en réponse
à ce problème de la resténose intrastent. Schématique-
ment, les DES sont constitués d’une plateforme métal-
lique identique à celle des BMS, recouverte d’un polymère
qui délivre une drogue cytotoxique inhibant la proliféra-
tion néo-intimale source de resténose. Trois DES sont
commercialisés en France, le premier délivrant du siro-
limus (Cypher®, Cordis), le second du paclitaxel (Taxus®,
Boston Scientifics®), le troisième l’ABT-578, analogue
du sirolimus (Endeavor®, Medtronic). Les deux premiers,
bénéficiant de l’antériorité, ont la validation scientifique la
plus forte, et préviennent cette prolifération néo-intimale
de la manière la plus prononcée. Les DES ont prouvé leur
capacité à réduire le taux de resténose chez le diabétique
par rapport aux BMS, mais même après implantation de
DES, les diabétiques ont toujours un risque de resténose
plus important que les non diabétiques (3). L’ensemble
de ces données a fait que, en France, ces trois DES sont
inscrits à la liste des produits et prestations remboursables
en cas de diabète, à l’exclusion toutefois de certaines situa-
tions, telles que la revascularisation en phase aiguë d’in-
farctus du myocarde.
Une étude ancillaire de l’essai ARTS-II s’est intéressée à
l’impact de la revascularisation par ICP avec utilisation
d’un DES au sirolimus sur les événements cardiaques et
cérébrovasculaires majeurs (MACCE) à 1 an puis à 3 ans
chez des patients diabétiques pluritronculaires (18). Cent
cinquante-neuf patients traités par DES ont été comparés
à une population témoin historique correspondant aux
112 patients traités par BMS et aux 96 patients traités par
PC inclus dans ARTS. Alors que les patients inclus dans
ARTS-II étaient porteurs de lésions plus étendues, la survie

136
Métabolismes Hormones Diabètes et Nutrition (XII), n°3, mai-juin 2008
Mise au point
Mise au point
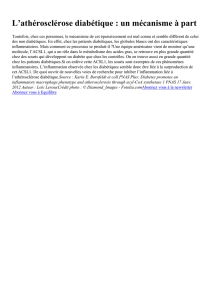
60
0
83,8 %p = 0,22
p < 0,001
Temps (mois)
Survie indemne
d'événement clinique (%)
80,6 %
66,0 %
100
65
70
75
80
85
90
95
6 12 18 24 30 36
ARTS II SES
ARTS I CABG ARTS I PCI
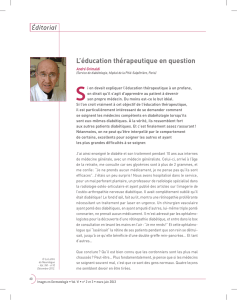
Figure 2. Courbes de Kaplan-Meier à trois ans chez les patients dia-
bétiques de ARTS et ARTS-II (adapté de 18).
SES : sirolimus eluting stent – CABG : coronary artery bypass graft
surgery – PCI : percutaneous coronary intervention.
à 1 an puis 3 ans sans MACCE fut comparable dans le bras
DES (ARTS-II) et dans le bras PC de ARTS, et signifi-
cativement meilleure que dans le bras BMS de ARTS
(figure 2). 12,6% des patients traités par DES ont nécessité
une ou des nouvelles revascularisations à un an contre 4,2%
des sujets traités par PC (p = 0,027) et 22,3% des patients
traités par BMS (p = 0,046). Ces résultats ne permettent
pas de conclusion définitive du fait d’un certain nombre
de biais (absence de randomisation, manque de puissance,
absence de suivi à long terme…). Ils semblent toutefois
réduire peu à peu la frontière séparant PC et ICP avec DES
chez les pluritronculaires diabétiques. Néammoins, l’im-
pact exact de l’emploi des DES sur la mortalité à moyen
et long terme, dans cette indication, et par comparaison à
la chirurgie de PC, reste toujours à définir, d’autant plus
que l’utilisation à grande échelle de ces nouvelles endopro-
thèses a fait naître des doutes quant à leur innocuité.
Le fait de ralentir la prolifération néo-intimale à la face
endoluminale de ces endoprothèses a bien permis de limiter
la resténose mais a également prolongé leur durée d’endo-
thélialisation, quelquefois incomplète au bout d’un an alors
qu’elle était obtenue en moyenne au bout d’un mois avec
les BMS, exposant à un risque de thrombose tardive. La
description des premiers cas, associés à une morbimortalité
majeure et survenant principalement lors de l’arrêt des anti-
agrégants plaquettaires, a soulevé une vaste polémique au
sein de la communauté cardiologique. Des résultats contra-
dictoires ont été publiés. Après maintenant plusieurs années
de recul et l’uniformisation de la définition des thromboses
de stents, les données les plus récentes sur le sujet, issues soit
d’une vaste méta-analyse (19) regroupant 18000 patients
inclus dans 38 essais cliniques, soit de registres plus en
adéquation avec la pratique quotidienne regroupant un
peu plus de 10500 patients (20), sont concordantes et ne
mettent pas en évidence de risque accru lié aux DES. Ceci à
condition de poursuivre une double antiagrégation plaquet-
taire pendant au moins un an après implantation de DES,
conformément aux recommandations des sociétés savantes
nord-américaines et européennes à ce sujet (21, 22).
La prise en charge médicale du patient
diabétique
Il ne faut pas oublier qu’en addition aux bénéfices poten-
tiels de la revascularisation, la prise en charge agressive
des facteurs de risque cardiovasculaire et diverses inter-
ventions pharmacologiques permettent une réduction
significative des MACCE. Ainsi, l’adjonction d’inhibi-
teurs des glycoprotéines IIbIIIa (anti-Gp IIbIIIa) lors de
la prise en charge invasive des syndromes coronariens
aigus sans sus-décalage du segment ST est-elle recom-
mandée chez le diabétique, conférant un avantage en
termes de survie (23). Le ramipril a prouvé sa capacité
à réduire les événements cardiovasculaires majeurs chez
le diabétique ayant un autre facteur de risque ou ayant
déjà présenté un événement cardiovasculaire (24). La
simvastatine et l’atorvastatine réduisent également les
événements cardiovasculaires majeurs chez le diabétique,
en prévention primaire et indépendamment du niveau de
LDL-cholestérol initial (25, 26). Enfin, chez les diabéti-
ques de type 2, le contrôle glycémique optimal après ICP
permet de diminuer le taux de nouvelle revascularisation
du vaisseau cible à une valeur quasi identique à celle
observée chez les non diabétiques (27).
La plupart de ces données n’étaient pas ou venaient d’être
publiées lorsque les essais thérapeutiques de revascula-
risation détaillés plus haut ont été conduits. Chez le
diabétique, on ne sait donc pas aujourd’hui quel est le
bénéfice d’une revascularisation comparée à une telle
stratégie médicale agressive, ni en cas de revascularisa-
tion chirurgicale ou percutanée, quel est l’impact exact de
ces mesures pharmacologiques.
Conclusion et perspectives
Les progrès techniques constants dans le domaine des ICP,
avec la généralisation des BMS durant les années 1990
puis celle des DES depuis quelques années, semblent petit
à petit réduire l’écart entre revascularisation coronarienne
chirurgicale et percutanée. Devant des lésions d’athéro-
sclérose coronaire diffuses, sévères, atteignant le TCG,
qui sont observées plus souvent chez les diabétiques, la
chirurgie de PC reste encore la méthode de référence.
En effet, à l’exception de situations telles que les lésions
focales mono- voire bitronculaires, ou la recanalisation de
l’artère occluse en phase aiguë d’infarctus du myocarde
pour lesquelles le choix de l’ICP s’est imposé, les données
scientifiques comparant PC et ICP à notre disposition chez
les pluritronculaires diabétiques, issues d’analyse de sous-
groupes d’essais randomisés, souffrent encore de trop de
limitations pour pouvoir recommander la revascularisation
endoluminale en première intention (figure 3).

137
Métabolismes Hormones Diabètes et Nutrition (XII), n°3, mai-juin 2008
Mise au point
Mise au point
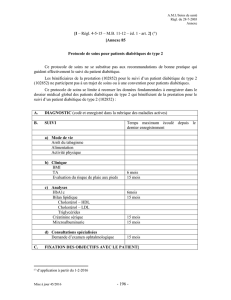
Figure 3. Choix du mode de revascularisation chez les patients dia-
bétiques (adapté de 3).
En cas d’ICP, implantation d’un DES fortement recommandée (à
l’exception de l’infarctus du myocarde en phase aiguë).
Patient diabétique avec indication de revascularisation coronaire
Sténose du TCG
≥ 50% Tritronculaire
ou
bitronculaire
avec sténose IVA
proximale ≥ 70%
Monotronculaire
ou
bitronculaire
sans sténose IVA
proximale
Haut risque
PC recommandé PC recommandé
en première
intention, ICP
alternative
raisonnable
ICP
recommandée
Aucune
stratégie
recommandée,
choix au cas
par cas
Les DES, réduisant le taux de resténose et donc la néces-
sité de revascularisations répétées, principale faiblesse, du
moins à court terme, des ICP par rapport aux PC, et les
résultats de la prise en charge médicale globale du patient
diabétique ont fait naître la nécessité d’essais randomisés
dédiés aux diabétiques comparant ces stratégies modernes.
Deux de ces essais, internationaux, sont actuellement en
cours et aideront probablement à préciser la stratégie théra-
peutique optimale. Tout d’abord, l’étude BARI 2 D (Bypass
Angioplasty Revascularization Investigation 2 Diabetes)
comparera, chez des patients diabétiques de type 2 avec
des lésions coronaires stables angiographiquement docu-
mentées, selon un plan factoriel 2 x 2, revascularisation
associée à un traitement médical agressif versus traite-
ment médical agressif seul, et simultanément deux stra-
tégies intensives de contrôle glycémique. Les inclusions
ont pris fin en mars 2005 avec un total de 2368 patients
inclus. Le critère de jugement principal sera la mortalité
toutes-causes à 5 ans. Enfin, l’essai FREEDOM (Future
Revascularization Evaluation in patients with Diabetes
mellitus: Optimal Management of Multivessel disease),
dont les inclusions sont en cours, comparera les MACCE
à 1 an puis la mortalité à 5 ans chez environ 1500 patients
diabétiques pluritronculaires, revascularisés soit par ICP
avec DES et abciximab (anti-Gp IIbIIIa), soit par PC.
Références bibliographiques
1.
Bonow RO, Gheorghiade M. The diabetes epidemic: a national and global
crisis. Am J Med 2004;116(Suppl.5A):2S-10S.
2.
Lee CD, Folsom AR, Pankow JS et al. Cardiovascular events in diabetic and
nondiabetic adults with or without history of myocardial infarction. Circulation.
2004;109(7):855-60.
3.
Flaherty JD, Davidson CJ. Diabetes and coronary revascularization. JAMA.
2005;293(12):1501-8.
4.
Berry C, Tardif JC, Bourassa MG. Coronary heart disease in patients with
diabetes: part II: recent advances in coronary revascularization. J Am Coll
Cardiol 2007;49(6):643-56.
5.
Nesto RW. Correlation between cardiovascular disease and diabetes melli-
tus: current concepts. Am J Med 2004;116(Suppl.5A):11S-22S.
6.
Creager MA, Luscher TF, Cosentino F et al. Diabetes and vascular disease:
pathophysiology, clinical consequences and medical therapy: Part I. Circula-
tion 2003;108(12):1527-32.
7.
Waller BF, Palumbo PJ, Lie JT et al. Status of the coronary arteries at
necropsy in diabetes mellitus with onset after age 30 years. Analysis of 229
diabetic patients with and without clinical evidence of coronary heart disease
and comparison to 183 control subjects. Am J Med 1980;69(4):498-506.
8.
Lemp GF, Vander Zwaag R, Hughes JP et al. Association between the seve-
rity of diabetes mellitus and coronary arterial atherosclerosis. Am J Cardiol
1987;60(13):1015-9.
9.
Ledru F, Ducimetiere P, Battaglia S et al. New diagnostic criteria for diabe-
tes and coronary artery disease: insights from an angiographic study. J Am Coll
Cardiol 2001;37(6):1543-50.
10.
Mak KH, Faxon DP. Clinical studies on coronary revascularization in
patients with type 2 diabetes. Eur Heart J 2003;24(12):1087-103.
11.
Abaci A, Oguzhan A, Kahraman S et al. Effect of diabetes mellitus on for-
mation of coronary collateral vessels. Circulation 1999;99(17):2239-42.
12.
Moreno PR, Murcia AM, Palacios IF et al. Coronary composition and
macrophage infiltration in atherectomy specimens from patients with diabetes
mellitus. Circulation 2000;102(18):2180-4.
13.
Comparison of coronary bypass surgery with angioplasty in patients with
multivessel disease. The Bypass Angioplasty Revascularization Investigation
(BARI) Investigators. N Engl J Med 1996;335(4):217-25.
14.
Brophy JM, Belisle P, Joseph L. Evidence for use of coronary stents. A hie-
rarchical bayesian meta-analysis. Ann Intern Med 2003;138(10):777-86.
15.
Mehran R, Dangas G, Abizaid AS et al. Angiographic patterns of in-stent
restenosis: classification and implications for long-term outcome. Circulation
1999;100(18):1872-8.
16.
Legrand VM, Serruys PW, Unger F et al. Three-year outcome after coro-
nary stenting versus bypass surgery for the treatment of multivessel disease.
Circulation 2004;109(9):1114-20.
17.
Sedlis SP, Morrison DA, Lorin JD et al. Percutaneous coronary interven-
tion versus coronary bypass graft surgery for diabetic patients with unstable
angina and risk factors for adverse outcomes with bypass: outcome of diabetic
patients in the AWESOME randomized trial and registry. J Am Coll Cardiol
2002;40(9):1555-66.
18.
Macaya C, Garcia-Garcia HM, Colombo A et al. One-year results of coro-
nary revascularization in diabetic patients with multivessel coronary artery
disease. Sirolimus stent versus coronary artery bypass surgery and bare metal
stent: insights from ARTS-II and ARTS-I. Eurointervention 2006;2:69-76.
19.
Stettler C, Wandel S, Allemann S et al. Outcomes associated with drug-
eluting and bare-metal stents: a collaborative network meta-analysis. Lancet
2007;370(9591):937-48.
20.
Marzocchi A, Saia F, Piovaccari G et al. Long-term safety and efficacy
of drug-eluting stents: two-year results of the REAL (REgistro AngiopLastiche
dell'Emilia Romagna) multicenter registry. Circulation 2007;115(25):3181-8.
21.
Smith SC, Feldman TE, Hirshfeld JW et al. ACC/AHA/SCAI 2005 guide-
line update for percutaneous coronary intervention: a report of the American
College of Cardiology/American Heart Association Task Force on Practice
Guidelines (ACC/AHA/SCAI Writing Committee to Update 2001 Guidelines for
Percutaneous Coronary Intervention). Circulation 2006;113(7):e166-286.
22.
Silber S, Albertsson P, Aviles FF et al. Guidelines for percutaneous coro-
nary interventions. The Task Force for Percutaneous Coronary Interventions of
the European Society of Cardiology. Eur Heart J 2005;26(8):804-47.
23.
Roffi M, Chew DP, Mukherjee D et al. Platelet glycoprotein IIb/IIIa inhibi-
tors reduce mortality in diabetic patients with non-ST-segment-elevation acute
coronary syndromes. Circulation 2001;104(23):2767-71.
24.
Effects of ramipril on cardiovascular and microvascular outcomes in
people with diabetes mellitus: results of the HOPE study and MICRO-HOPE
substudy. Heart Outcomes Prevention Evaluation Study Investigators. Lancet
2000;355(9200):253-9.
25.
Collins R, Armitage J, Parish S et al. MRC/BHF Heart Protection Study of
cholesterol-lowering with simvastatin in 5963 people with diabetes: a rando-
mised placebo-controlled trial. Lancet 2003;361(9374):2005-16.
26.
Colhoun HM, Betteridge DJ, Durrington PN et al. Primary prevention of
cardiovascular disease with atorvastatin in type 2 diabetes in the Collabora-
tive Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-
controlled trial. Lancet 2004;364(9435):685-96.
27.
Corpus RA, George PB, House JA et al. Optimal glycemic control is asso-
ciated with a lower rate of target vessel revascularization in treated type II
diabetic patients undergoing elective percutaneous coronary intervention. J Am
Coll Cardiol 2004;43(1):8-14.
1
/
5
100%