thématique D

RÉSUMÉ SUMMARY
Dossier
tmiqu
Le Courrier de la Transplantation - Volume VIII - n
o 1 - janvier-février-mars 2008
33
Néphrotoxicité
Coordinateur :
D. Anglicheau
Mesures de prévention et de traitement
de la néphrotoxicité des anticalcineurines
en transplantation cardiaque
Prevention and treatment of calcineurin inhibitors-
induced nephrotoxicity in heart transplant patients
L. Sebbag*●
* Pôle de transplantation cardiaque, hôpital Louis-
Pradel, Lyon.
S
i les anticalcineurines, et notam-
ment la ciclosporine, ont révo-
lutionné et permis le succès
des transplantations cardiaques, il est
aujourd’hui admis que le béné ce de
ces traitements à long terme est limité
par leur néphrotoxicité. Les progrès de
la prise en charge ont permis d’améliorer
notablement la mortalité initiale post-
transplantation cardiaque au cours des
quinze dernières années. En revanche,
Si les inhibiteurs de la calcineurine ont participé au
succès de la transplantation, ils demeurent associés
à une comorbidité sévère, comme l’illustre la néphro-
toxicité. Les données de registres rapportent une
prévalence allant de 6 à 8 % d’insuf sance rénale
sévère chez les transplantés cardiaques, 1 % des cas
nécessitant une dialyse. Les facteurs prédictifs identi-
és sont l’âge, le diabète, l’altération préexistante de
la fonction rénale et l’instabilité hémodynamique. La
prévention fait appel à l’amélioration de l’évaluation
de la fonction rénale prétransplantation, à l’utilisa-
tion d’un traitement d’induction, à la diminution
des inhibiteurs de la calcineurine, à l’utilisation de
nouveaux immunosuppresseurs (inhibiteurs du signal
de prolifération). Le rôle éventuel de polymorphismes
génétiques et l’intérêt de mesures de prévention de
cette iatrogénie seront également discutés.
Mots-clés : Néphrotoxicité – Ciclosporine –
Inhibiteurs de la calcineurine – Transplantation
cardiaque – Prévention.
While anticalcineurin agents have succeeded in
making transplantation a reality, they are still asso-
ciated with severe morbidity as illustrated by nephro-
toxicity. Historical and recent registry data report
a 6 to 8% prevalence of severe renal dysfunction
in HT patients with 1% of them requiring kidney
transplantation. Among the predictive factors are
identi ed older recipients, diabetes, pretransplant
elevated creatinine or hemodynamic instability. Preven-
tion is suggested to be achieved by different ways:
improving pretransplant renal evaluation, use of induc-
tion therapy, tailorized anticalcineurin use (reduction
of initial or long term exposure, pharmacokinetic
monitoring), use of new immunosuppressive agents
(proliferation signal inhibitors). Potential role of genetic
polymorphism and protection against iatrogenesis to
help reduce nephrotoxicity are discussed.
Keywords:
Nephrotoxicity
–
Cyclosporin
–
Calcineurin inhibitors
–
Heart transplantation
–
Prevention.
la mortalité à long terme reste déses-
pérément stable, avec une survie dimi-
nuant de 3,4 % par an, même au-delà des
quinze années post-transplantation, selon
les dernières données du registre de la
Société internationale de transplantation
cardiaque et pulmonaire (ISHLT) [1].
Avec une médiane de survie de 10 ans et
une demi-vie de 13 ans pour les patients
survivant à leur première année post-
transplantation, la durée de vie postgreffe
s’est notablement allongée, permettant
le développement de la morbidité post-
transplantation.

Dossier
tmiqu
Le Courrier de la Transplantation - Volume VIII - n
o 1 - janvier-février-mars 2008
34
ÉVALUATION DE L’INSUFFISANCE
RÉNALE CHEZ LE TRANSPLANTÉ
CARDIAQUE
Si différents marqueurs ont été évalués,
comme la cystatine C ou l’urinary
Retinol Binding Protein (uRBP), la
plupart des équipes de transplantation
cardiaque suivent l’évolution de la
déchéance rénale par la créatininémie
et/ou la clairance de créatinine calculée
par la formule de Cockcroft ou du
MDRD.
La publication de N.O. Camara et al.
dans le Lancet en 2001 (2) mettait en
avant l’intérêt de la mesure de l’uRBP,
dont le taux témoignait de l’atteinte
tubulo-interstitielle et semblait tout à
fait corrélé au développement de l’in-
sufsance rénale post-transplantation
cardiaque. Cette étude prospective
concernait (seulement !) 36 patients. Il
n’y a pas eu d’autres études conrma-
tives ni d’utilisation plus systématique
de ce paramètre dans le suivi de nos
patients transplantés cardiaques.
PRÉVALENCE DE L’INSUFFISANCE
RÉNALE CHEZ LE TRANSPLANTÉ
CARDIAQUE
Selon les dernières données du registre
de la Société internationale de transplan-
tation cardiaque et pulmonaire, l’insuf-
fisance rénale significative survient
chez 14 % des patients. Elle peut être
dénie par une créatinine supérieure à
2,5 mg/dl (8 % des patients), par une
prise en charge en dialyse au long cours
(5 % des patients) ou par une transplan-
tation rénale (1 % des patients) [1]. Ces
données récentes sont malheureusement
peu différentes de celles déjà raportées
par D.J. Goldstein et al. en 1997 (3), qui
décrivaient une élévation de la créatinine
chez plus d’un tiers des patients dans les
6 premiers mois et un recours à l’hémo-
dialyse chez 6,5 % d’entre eux.
Un certain nombre de facteurs ont été
dénis comme prédictifs du dévelop-
pement de cette insuffisance rénale
post-transplantation cardiaque dès la
cinquième année postgreffe (tableau).
On retiendra la survenue d’un diabète
chez le receveur, un âge élevé, une insuf-
sance rénale ou une instabilité hémo-
dynamique prétransplantation.
La prise d’anticalcineurines n’est pas
incluse dans les données du registre de
l’ISHLT, mais elle est probablement
implicite derrière l’augmentation de
l’insufsance rénale chez des patients
immunisés présentant vraisemblable-
ment plus de rejets et justiant le main-
tien de taux d’immunosuppresseurs
anticalcineurines plus élevés que pour
les autres patients.
D’autres auteurs, indépendants du
registre de l’ISHLT, ont mis en avant
des facteurs prédictifs. B. Lindelow et al.
(4) identiaient ainsi l’âge du receveur
comme un important facteur prédictif
de l’insufsance rénale post-transplan-
tation.
Le développement de l’insuffisance
rénale terminale chez le greffé cardiaque
est extrêmement préoccupant car entaché
d’une très lourde morbi-mortalité (5).
MESURES DE PROTECTION
PROPOSÉES
Face à cette apparente inéluctabilité, les
équipes de transplantation thoracique,
et donc cardiaque, ont développé au l
des années des stratégies permettant
de réduire et/ou d’améliorer la prise
en charge de ces patients insufsants
rénaux.
Amélioration du screening prégreffe
Le premier élément est une meilleure
considération de l’insufsance rénale
prétransplantation par une prise en
charge collaborative entre néphrologues
et cardiologues de transplantation des
patients présentés à la greffe cardiaque.
Cette approche, associée à une évalua-
tion fonctionnelle rénale, est indiscu-
tablement utile dans l’orientation du
patient fragile vers une prise en charge
adaptée : contre-indication à la greffe,
greffe rénale associée, immunosuppres-
sion personnalisée post-transplantation.
C’est vers cette personnalisation de
l’immunosuppression postgreffe que
se sont tournées le plus grand nombre
d’équipes an de limiter l’insufsance
rénale.
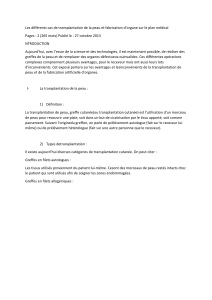
Tableau. Facteurs de risque pour le développement d’une insufsance rénale sévère dans les
5 ans suivant une greffe cardiaque réalisée entre avril 1994 et juin 2001 (n = 11 145) [1].
Variable Risque relatif p IC95
Diabète chez le receveur 1,47 < 0,0001 1,33-1,62
Année de gree : 1994/1995 1,24 0,0008 1,09-1,40
Année de gree : 1996/1997 1,22 0,001 1,09-1,38
Receveur avec infection justiant une antibiothérapie i.v.
dans les 2 semaines précédant la gree 1,22 0,0047 1,06-1,40
Inotropes i.v. lors de la gree 1,19 < 0,0001 1,10-1,29
Année de gree : 1998/1999 1,17 0,0084 1,04-1,32
HTA prégree chez le receveur 1,15 0,0011 1,06-1,25
Âge du receveur (linéaire) < 0,0001
Poids du receveur (linéaire) < 0,0001
Créatinine du receveur (linéaire) < 0,0001
PRA (panel reactive antibody) du receveur (linéaire) 0,0047
Poids du donneur (inverse) 0,049

Dossier
tmiqu
Le Courrier de la Transplantation - Volume VIII - n
o 1 - janvier-février-mars 2008
35
Traitement d’induction
Concernant la présence ou l’absence
d’un traitement d’induction, il n’existe
pas d’étude randomisée répondant de
manière indiscutable au rôle joué par
l’induction par ATG (antithymocyte
globulin) ou par les anti-IL-2R sur la
réduction de la néphrotoxicité des inhibi-
teurs de la calcineurine. M. Cantarovich
et al. (6) ont cependant rapporté que la
prolongation de l’induction par ATG
a permis de différer l’introduction de
la ciclosporine de quelques jours dans
le cas d’une insufsance rénale immé-
diatement postopératoire. Les auteurs
postulent que ce décalage dans l’intro-
duction des inhibiteurs de la calcineurine
a épargné le rein. La même équipe a
proposé et testé chez 6 patients l’utili-
sation des antagonistes de récepteurs à
l’IL-2 (à distance de la greffe) comme
substitution à la ciclosporine (7).
Personnalisation de l’utilisation
de la ciclosporine
Réduction des doses initiales
L’essai clinique multicentrique français
Low Ciclo (8), dont les résultats à un an
sont attendus en 2008, a été déni de
manière à répondre à cette question. La
sécurité d’utilisation de plus faibles doses
de ciclosporine pendant les premiers
mois postgreffe cardiaque ainsi que le
bénéce sur la fonction rénale ont été
évalués. Selon l’analyse intermédiaire à
6 mois, l’introduction d’une faible dose
de ciclosporine dans les premiers jours
suivant la greffe semble améliorer la
fonction rénale. Cette tendance demande
à être conrmée avec l’analyse nale à
12 mois.
Monitoring pharmacocinétique
La mesure de la concentration plasma-
tique de ciclosporine à 2 heures de sa
prise a, par exemple, été proposée, avec
des arguments scientiques valides, pour
en limiter la néphrotoxicité. J.B. Barnard
et al. (9) rapportent ainsi, à 12 mois
d’une transplantation cardiaque, l’amé-
lioration du débit de ltration glomé-
rulaire (54 ± 14 versus 70 ± 23 ml/mn
[p < 0,004]) chez les 28 patients suivis
par le taux résiduel et le C2.
●
●
Réduction de l’exposition tardive
Évidemment, à distance d’une greffe
cardiaque, toutes les équipes devant faire
face au développement d’une insuf-
sance rénale commencent par réduire
les doses quotidiennes des inhibiteurs
de calcineurine. Cette habitude logique
est cependant souvent trop tardive pour
être réellement bénéque, même si les
seuils de réaction se sont améliorés au
l des années !
Introduction des nouveaux
immunosuppresseurs
L’arrivée d’immunosuppresseurs diffé-
rents, comme le mycophénolate mofétil
(MMF) dans les années 1995-2000 puis
les inhibiteurs de la protéine mTOR,
nous offrent aujourd’hui des thérapeu-
tiques qui permettent, tout en réduisant
l’exposition à la ciclosporine, de garder
une efcacité immunosuppressive satis-
faisante.
Mycophénolate mofétil (Cellcept®)
L’introduction du MMF en lieu et place
de l’azathioprine a sans doute été un
tournant dans la capacité à réduire puis à
arrêter l’exposition à la ciclosporine (10).
Deux situations ont été analysées.
Utilisation du MMF pour prévenir
l’installation de l’insufsance rénale.
I.M. Hamour et al. (11) ont ainsi
récemment comparé, dans une série de
240 patients, l’association de faibles
doses de ciclosporine à du MMF versus
ciclosporine et azathioprine. Le bénéce
à l’issue de la première année postgreffe
est signicativement en faveur du MMF
(créatinine plasmatique : 133 ± 45 versus
155 ± 46 µmol/l [p < 0,0004]).
Introduction tardive du MMF alors
que l’insuffisance rénale est déjà
installée. G. Dureau et al. (12) rappor-
taient en 2000 leur expérience de sevrage
de la ciclosporine chez 8 patients trans-
plantés cardiaques après introduction du
MMF. Dans cette petite série concernant
des patients transplantés en moyenne
8,6 ans auparavant et avec une créati-
ninémie située entre 263 et 409 µmol/l,
la réduction progressive puis l’arrêt de
●
●
✓
✓
la ciclosporine a permis l’améliora-
tion de la fonction rénale chez 7 des
8 patients.
Inhibiteurs de la protéine mTOR :
sirolimus (Rapamune®) ou évérolimus
(Certican®)
Ils représentent l’autre piste thérapeu-
tique explorée aujourd’hui pour réduire
la néphrotoxicité de la ciclosporine.
J. Hunt et al. (13) ont ainsi rapporté
en 2005 le bénéce du remplacement
de la ciclosporine par du sirolimus
chez 80 greffés cardiaques, 4,78 ans
en moyenne post-transplantation. En
moyenne, 304 jours après la conversion,
la créatininémie s’est améliorée, passant
de 2,04 ± 0,57 mg/dl préconversion à
1,64 ± 0,48 mg/dl (p < 0,001).
H.B. Lehmkuhl et al. (14) ont publié une
étude observationnelle démontrant la
faisabilité d’une réduction de l’exposi-
tion à la ciclosporine par l’introduction
d’évérolimus. D’autres équipes, notam-
ment françaises, ont partagé cette expé-
rience (15).
M. Rothenburger et al. (16) ont proposé
et évalué l’arrêt complet des inhibi-
teurs de la calcineurine avec introduc-
tion de l’évérolimus. Ils démontrent
sur une série de 60 patients, plus de
5 ans après leur transplantation, que
l’arrêt des inhibiteurs de la calcineu-
rine est possible et permet l’améliora-
tion de la fonction rénale. La médiane
de clairance de créatinine (formule de
Cockcroft-Gault) a augmenté, passant
de 39,6 ml/mn/1,73 m2 (IQR 25/75 :
28,0-48,2 ml/mn/1,73 m2) à 60,7 ml/
mn/1,73 m
2
(IQR 25/75 : 46,0-77,2 ml/
mn/1,73 m
2
), 3 mois après la conversion
(p = 0,018).
La gestion d’une immunosuppression
de novo sans inhibiteur de la calcineu-
rine reste extrêmement anecdotique en
transplantation cardiaque. L’expérience
de B. Meiser et al. (17) proposant une
immunosuppression d’emblée à base de
sirolimus et de MMF n’est rapportée que
pour 8 patients, avec un taux de succès
de 100 %...
●

Dossier
tmiqu
Le Courrier de la Transplantation - Volume VIII - n
o 1 - janvier-février-mars 2008
36
NOUVELLES PISTES
Il serait beaucoup plus utile de pouvoir
identier a priori des sous-groupes de
patients à risque chez lesquels ces modi-
cations thérapeutiques pourraient être
encouragées plutôt que de courir après
une amélioration de la créatinine.
Les études de polymorphisme génique
constituent une nouvelle piste dans la
prise en charge de ces patients ainsi
que dans l’identication des groupes à
risque. C.C. Baan et al. (18) avaient, par
exemple, identié un polymorphisme sur
le gène du TGFβ-1, la présence d’une
proline au codon 10, dans leur analyse
menée chez 168 patients transplantés
cardiaques, associé à une accélération du
développement de l’insufsance rénale.
Nous avons également pu démontrer
que la présence de polymorphismes
mononucléotidiques était prédictive de
l’installation d’une insufsance rénale
terminale (19).
Enn, il ne faut pas oublier les situa-
tions où l’insufsance rénale apparaît
comme une complication iatrogène en
transplantation cardiaque avec notam-
ment l’augmentation des coronarogra-
phies et des examens angiographiques
iodés. La néphropathie induite par les
produits de contraste est l’une des situa-
tions fréquemment redoutées. Face à
cette situation et bien que le débat soit
toujours ouvert sur la meilleure façon
de réduire la toxicité de ces agents de
contraste, la plupart des équipes de
transplantation thoracique ont recours,
conformément à la publication du Lancet
(20), à l’addition de N-acétyl cystéine
associée à une hydratation salée entou-
rant la réalisation du geste angiogra-
phique. La diminution des quantités
d’iode dans les coronarographies stan-
dard a également été un facteur favorable
dans cette prévention.
D’autres pistes intéressantes ont été
proposées, mais elles sont soit unique-
ment rétrospectives, comme l’effet protec-
teur des statines dans le développement
de l’insufsance rénale chronique (21),
soit non évaluées chez l’homme, comme
l’utilisation d’agents anti-ischémiques
tels que la trimétazidine (22).
CONCLUSION
Face à des données de registres préoc-
cupantes, nous avons dessiné dans cette
mise au point les pistes aujourd’hui utili-
sées ou s’offrant maintenant à nous pour
améliorer la qualité et la durée de vie de
nos patients transplantés. De nouveaux
immunosuppresseurs, de nouvelles
méthodes de dépistage et surtout une
collaboration transversale renforcée en
sont les clés de voûte. ■
RéféRences
bibliogRaphiques
1. Taylor DO, Edwards LB, Boucek MM et al.
Registry of the International Society for Heart and
Lung Transplantation: twenty-fourth ofcial adult
heart transplant report. J Heart Lung Transplant
2007;26(8):769-81.
2. Camara NO, Matos AC, Rodrigues DA, Pereira
AB, Pacheco-Silva A. Early detection of heart
transplant patients with increased risk of cyclo-
sporin nephrotoxicity. Lancet 2001;357:856-7.
3. Goldstein DJ, Zuech N, Sehgal V, Weinberg AD,
Drusin R, Cohen D. Cyclosporin-associated end-
stage nephropathy after cardiac transplantation:
incidence and progression. Transplantation 1997
15;63(5):664-8.
4. Lindelow B, Bergh CH, Herlitz H, Waagstein F.
Predictors and evolution of renal function during
9 years following heart transplantation. J Am Soc
Nephrol 2000;11(5):951-7.
5. Villar E, Boissonnat P, Sebbag L et al. Poor
prognosis of heart transplant patients with end-
stage renal failure. Nephrology Dialysis Transplan-
tation 2007;22(5):1383-9.
6. Cantarovich M, Giannetti N, Barkun J, Cecere R.
Antithymocyte globulin induction allows a
prolonged delay in the initiation of cyclosporin in
heart transplant patients with postoperative renal
dysfunction. Transplantation 2004;78(5):779-81.
7. Cantarovich M, Giannetti N, Routy JP, Cecere R.
Calcineurin inhibitor substitution (“retirement”)
with anti-CD25 monoclonal antibodies: a novel
strategy in long-term heart transplant patients with
progressive renal dysfunction. Transplantation
2006;82(Suppl. 3):552-3.
8. Boissonnat P, Gaillard S, Noël-Baron F et
al. Étude multicentrique française randomisée
évaluant le bénéce sur la fonction rénale d’une
posologie allégée en ciclosporine en transplan-
tation cardiaque : résultats à 6 mois. Communi-
cation 27th Annual meeting of the International
Society for Heart and Lung Transplantation San
Francisco, 2007.
9. Barnard JB, Thekkudan J, Richardson S et al.
Cyclosporin proling with C2 and C0 monitoring
improves outcomes after heart transplantation.
J Heart Lung Transplant 2006;25(5):564-8.
10. Kobashigawa J, Miller L, Renlund D et al.
A randomized active controlled trial of myco-
phenolate mofetil in heart transplant recipients.
Transplantation 1998;66(4):507-15.
11. Hamour IM, Lyster HS, Burke MM, Rose
ML, Banner NR. Mycophenolate mofetil may
allow cyclosporin and steroid sparing in de novo
heart transplant patients. Transplantation 2007;
83:570-6.
12. Dureau G, Obadia JF, Chuzel M, Boissonnat
P. Introduction of mycophenolate mofetil and
cyclosporin withdrawal in heart transplant patients
with progressive deteriorating renal function.
Transplantation Proceedings 2000;32:461-2.
13. Hunt J, Lerman M, Magee MJ, Dewey TM,
Herbert M, Mack MJ. Improvement of renal
dysfunction by conversion from calcineurin inhi-
bitors to sirolimus after heart transplantation.
J Heart Lung Transplant 2005;24(11):1863-7.
14. Lehmkuhl HB, Mai D, Dandel M et al. Obser-
vational study with everolimus (Certican®) in
combination with low-dose cyclosporin in de
novo heart transplant recipients. J Heart Lung
Transplant 2007;26(7):700-4.
15. Guillemain R. Insufsance rénale chez les
patients transplantés thoraciques. In : Recom-
mandations françaises d’utilisation de l’évéro-
limus en transplantation cardiaque. Éditions de
l’Interligne 2007.
16. Rothenburger M, Teerling E, Bruch C et al.
Calcineurin inhibitor-free immunosuppression
using everolimus (Certican
®
) in maintenance heart
transplant recipients: 6 months’ follow-up. J Heart
Lung Transplant 2007;26(3):250-7.
17. Meiser B, Reichart B, Adamidis I, Uberfuhr P,
Kaczmarek I. First experience with de novo calci-
neurin-inhibitor-free immunosuppression following
cardiac transplantation. Am J Transplant 2005;
5(4 Pt 1):827-31.
18. Baan CC, Balk AH, Holweg CTJ et al. Renal
failure after clinical heart transplantation is asso-
ciated with TGF-B1 codon10 gene polymorphism.
J Heart Lung Transplant 2000;19:866-72.
19. Sebbag L, Boissonnat P, Roussoulières A et al.
Cytokine polymorphism predicts early rejection
and late renal failure in heart transplant patients.
Transplant Int 2005;18(Suppl. 1):48.
20. Birck R, Krzossok S, Markowetz F et al. Acetyl
-
cysteine for prevention of contrast nephropathy:
meta-analysis. Lancet 2003;362:598-603.
21. Lubitz SA, Pinney S, Wisnivesky JP, Gass A,
Baran DA. Statin therapy associated with a
reduced risk of chronic renal failure after cardiac
transplantation. J Heart Lung Transplant 2007;
26(3):264-72.
22. Simon N, Tillement JP, Albengres E et al.
Potential interest of anti-ischemic agents for
limiting cyclosporin A nephrotoxicity. Int J Clin
Pharmacol Res 1997;17(4):133-42.
1
/
4
100%