S. Oudard - Longue Vie et Autonomie

1
Oncologie Urologique
du Sujet Agé
29 Mars 2013
Pr Stéphane OUDARD
Hôpital Européen Georges Pompidou, Paris
Assistance Publique – Hôpitaux de Paris
Impossible d'a!cher l'image. Votre ordinateur manque peut-être de mémoire pour ouvrir l'image ou l'image est endommagée. Redémarrez l'ordinateur,
puis ouvrez à nouveau le fichier. Si le x rouge est toujours a!ché, vous devrez peut-être supprimer l'image avant de la réinsérer.
Oncologie Urologique
Traitement
K de la prostate

2
Quel traitement choisir chez le
sujet âgé : CT ou HT ?
mCRPC
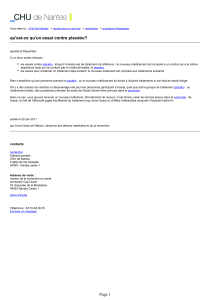
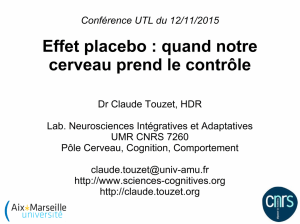
Inhibiteurs des micro-tubules
Docetaxel : stabilisation microtubules, arrêt phase G2M et induction P Bcl2
Inhibition de la polymérisation
Tubuline
α"
β"
Microtubule
Colchicine
Vinca Alcaloïdes
Taxanes
Inhibition de la depolymérisation

3
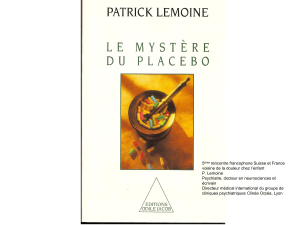
Stratification:
Niveau douleur
PPI ≥ 2 or AS ≥ 10
vs.
PPI < 2 or AS < 10
PS (IK)
≤70 vs. ≥ 80
Docetaxel 75 mg/m²/ 3 semaines
+ Prednisone 5mg x 2/j
Mitoxantrone 12 mg/m²/sem
+ Prednisone 5mg x 2/j
R
A
N
D
O
M
I
S
A
T
I
O
N
Docetaxel 30 mg/m²/semaine
5/6 sem + Prednisone 5mgx2/j
Durée traitement dans les 3 bras = 30 sem
Cancer de prostate hormono-résistant
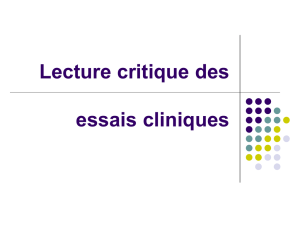
Etude TAX 327
M.A.Eisenberger , N Engl J Med 2004, 351:1502-12
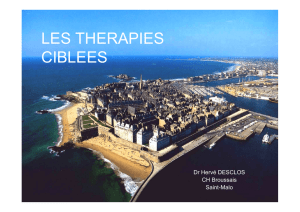
Mediane
survie Hazard
(mos) ratio P
Combiné: 18.2 0.83 0.03
D 3 sem: 18.9 0.76 0.009
D hebdo: 17.3 0.91 0.3
Mitoxantrone 16.4 – –
Mois
Probabilité de Survie
0 6 12 18 24 30
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Docetaxel /3 sem
Docetaxel hebdo
Mitoxantrone
Etude TAX327. Objectif principal : survie globale
M.A.Eisenberger , N Engl J Med 2004, 351:1502-12

4
Toxicité Hématologique
Grade 3-4 (%)
Docetaxel
3 semaines
Docetaxel
hebdomadaire Mitoxantrone
Traités 332 330 335
Anémie 5 5 2
Neutropénie 32,0 1,5 22
Neutropenie infection 3.0 0.0 0.9
Neutropénie fébrile 2.7 0.0 1.8
Décès septique 0.0 0.3 0.3
M.A.Eisenberger , N Engl J Med 2004, 351:1502-12
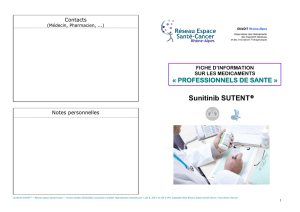
0.2 0.4 0.6 0.8 1 1.2 1.4
Intention de traiter
Age < 65 ans
Age ≥ 65 ans
Age ≥ 75 ans
Patient non algique
Patient algique
KPS ≥ 80
KPS ≤ 70
Hazard ratio
Docetaxel (J1,J21)
par rapport à Mitoxantrone
M.A.Eisenberger , N Engl J Med 2004, 351:1502-12
Survie Globale : Tax 327

5
Quand doit-on démarrer la
chimiothérapie ?
(Médiane) Docetaxel
(tous les 21 jours)
Mitoxantrone
(tous les 21 jours)
Patients
Symptomatiques 15,5 mois 13 mois
Patients
Asymptomatiques* 22,3 mois 20 mois
Tax 327 : Survie Globale
• Peut-on sélectionner pts en fonction dynamique du PSA : TD PSA ?
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
1
/
41
100%