2013 - Alger - Sunitinib et TED

Sunitinib et
TNE digestives
Emmanuel MITRY!
Département d'oncologie médicale!
Institut Curie!
Alger – Février 2013

Thérapies ciblées
- TNE bien différenciées, avancées et évolutives
- inhibiteur mTOR (everolimus)
- anti-angiogéniques
- sunitinib
- pazopanib
- bevacizumab

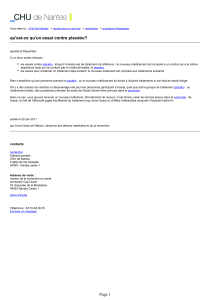
Sunitinib SUTENT®
• ITK anti-angiogénèse (PDGFR, VEGFR), c-KIT, RET, CSF1R, flt3
• Phase I (Faivre S et al. JCO 2006;24:25-36)
– Carcinose péritonéale d'une TE rectale
Avant Après


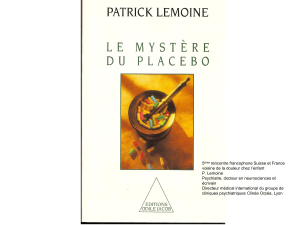
Design
A618111
Essai randomisé de phase III en double aveugle contre placebo
Randomisation 1/1
TE pancréatique bien différenciée
Métastatique ou avancée non accessible à la chirurgie
En progression (RECIST, 12 mois)
Bon EG OMS (0-1 SUN, 0-2 RAD)
Analogues SMS autorisés
Sunitinib vs placebo
5
 6
7
8
9
10
11
12
13
14
15
16
17
18
6
7
8
9
10
11
12
13
14
15
16
17
18
1
/
18
100%