Télécharger le poster

F.Garibaldi, M.Viala Trentini, N.Mazet, A.Suau, 0.Allice, C.Escare, Pr JP.Rouanet
Clinique Beausoleil Montpellier

DEFINITION
Tissu endométrial ectopique pénétrant:
•sous la surface du péritoine
•la paroi d’un organe pelvien
A une profondeur > 5 mm
Cornillie FJ. Deeply infiltrating pelvic endometriosis: histology and clinical significance.
Fertil. Steril. 1990.
Koninckx PR. Suggestive evidence that pelvic endometriosis is a progressive disease,
whereas deeply infiltrating endometriosis is associated with pelvic pain. Fertil. Steril. 1991.

HISTOLOGIE
Hyperplasie fibromusculaire
Foyers endométriosiques ADENOMYOME
Petites cavités
Vercellini P. Deep endometriosis: Definintion and Clinical management. J Am Assoc Gynecol Laparosc 2004.
Koninckx PR. Suggestive evidence that pelvic endometriosis is a progressive disease, whereas deeply infiltrating
endometriosis is associated with pelvic pain. Fertil. Steril. 1991.

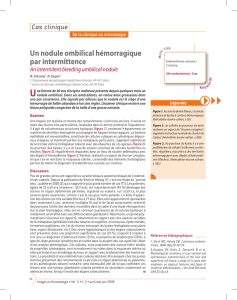
HISTOLOGIE
Glandes endométriales + stroma Tissu fibromusculaire
Prolifération musculaire lisse + Réaction fibreuse
Formation nodulaire solide
+
+
Vercellini P. Deep endometriosis: Definintion and Clinical management. J Am Assoc Gynecol Laparosc 2004.
Koninckx PR. Suggestive evidence that pelvic endometriosis is a progressive disease, whereas deeply infiltrating
endometriosis is associated with pelvic pain. Fertil. Steril. 1991.
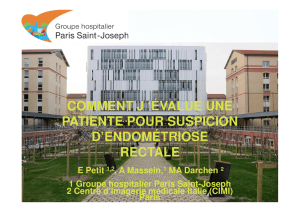
ENDOMETRIOSE SOUS PERITONEALE

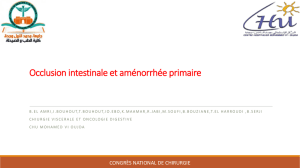
HISTOLOGIE
Implants surface séreuse
couche musculeuse
Prolifération musculaire lisse
Striction
Obstruction
Vercellini P. Deep endometriosis: Definintion and Clinical management. J Am Assoc Gynecol Laparosc 2004.
Koninckx PR. Suggestive evidence that pelvic endometriosis is a progressive disease, whereas deeply infiltrating
endometriosis is associated with pelvic pain. Fertil. Steril. 1991.
+
+
ENDOMETRIOSE VISCERALE
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
1
/
65
100%