Toxicité digestive des chimiothérapies

Toxicité digestive des
chimiothérapies
Pr Jean Trédaniel
Unité de cancérologie thoracique
Hôpital Saint-Louis

•Nausées & vomissements
•Diarrhée / constipation
•Mucite
•Douleur abdominale

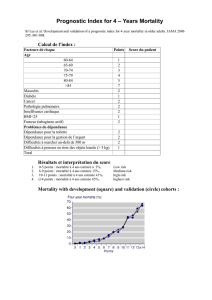
La nécessité d’améliorer la prise en charge des NVIC
1983 1995
(avant les antagonistes 5-HT3) (depuis les antagonistes 5-HT3)
Classement
1Vomissements Sensation de malaise (nausées)
2Sensation de malaise (nausées) Perte des cheveux
3 Perte des cheveux Vomissements
4 Penser à aller se faire traiter Constamment fatigué
5Durée du traitement à la clinique Nécessité d’une injection
6Nécessité d’une injection Constipation
7 Essoufflement Penser à aller se faire traiter
8 Constamment fatigué Affecte famille ou partenaire
9 Difficultés à dormir Se sentir déprimé, malheureux
10 Affecte famille ou partenaire Se sentir anxieux ou tendu
Effets indésirables les plus éprouvants de la chimiothérapie avant et
pendant l’époque des antagonistes des récepteurs 5-HT3
Br J Cancer 1997;76:1055-61
Eur J Cancer Clin Oncol 1983;19:203-8

Besoin non satisfait
Etude ANCHOR : Anti-Nausea Chemotherapy Registry
Objectif : déterminer l’incidence des nausées et vomissements aigus
et retardés et évaluer leur perception par le personnel soignant.
Méthodologie
•Etude internationale, prospective, multicentrique
• 300 patients adultes, n’ayant jamais reçu de chimiothérapie,
•298 patients éligibles
•Chimiothérapie moyennement ou hautement émétisante
•5-HT3 antagonistes : 97%
•Corticoïdes : 78%
•Auto-évaluation nausées et vomissements de J1 à J5
•Auto-évaluation de la qualité de vie à J0 et J6
Cancer 2004;100:2261-8

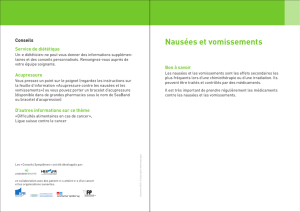
Perception des patients vs. Soignants
Pour les patients recevant une chimiothérapie hautement émétisante
0
10
20
30
40
50
60
NA VA NR VR
Patients
Soignants
Cancer 2004;100:2261-8
 6
7
8
9
10
11
12
13
14
6
7
8
9
10
11
12
13
14
1
/
14
100%