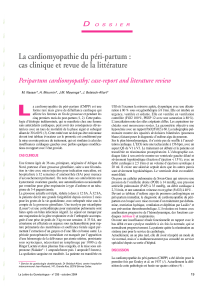
Cardiomyopathie du péripartum - Département d`Anesthésie du

Cardiomyopathie du péripartum
Staff d’Anesthésie du Lundi 20 Avril
2015
CHI Poissy St-Germain
Sarah Féray – Interne
!

Cas clinique
Madame TK, 36 ans, origine africaine
• Antécédents médicaux :
– Obésité IMC = 33
– Aucun FdR cardiovasculaire
• Antécédents obstétricaux :
– G3P3 :
– AVB en 2007 (4250g)
– AVB en 2009 (4950g)
– AVB en 2011 (5120g)
• Antécédents chirurgicaux : aucun
• Allergie : non connue
!

Histoire de la maladie
• Hospitalisé à 10 mois de sa dernière grossesse pour
décompensation cardiaque globale
• Se plaint depuis 2 mois d’une dyspnée d’effort
Examen clinique initial :
• Etat général conservé, apyrétique, TA 120/70, FC 90/min
• Dyspnée NYHA III
• Bruit du Coeur régulier, souffle systolique de 3/6ème mitral
• Signes d’insuffisance cardiaque gauche : crépitants aux
bases pulmonaires
• Signes d’insuffisance cardiaque droite : OMI,
hepatomegalie, reflux hépato-jugulaire

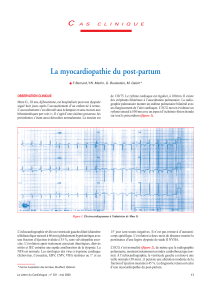
Examens complémentaires
• ECG : ryhtme sinusal à 90/min, trouble de la repolarisation non
spécifique
• Radio thorax : cardiomégalie, syndrome interstitiel accentué au
hile
• Biologie : normale sauf NTproBNP 2000 pg/ml, troponine
négative
• ETT :
VG dilaté - parois normotrophiques avec hypokinésie globale
FEVG = 33%
OG dilatée
Cavités droites non dilatés, pas d’HTAP
Fuite mitrale modérée

Diagnostic et PEC
• Insuffisance cardiaque globale sur cardiomyopathie
dilatée, hypokinétique, non connue auparavant chez une
patiente de 36 ans
• Hypothèse : cardiomyopathie dilatée liée à la grossesse
! Coroscanner : normal
! IRM cardiaque : cardiomyopathie dilatée non ischémique,
VG dilaté, FE à 33%.
Pas d’étiologie spécifique retrouvée = élimination diagnostic
différentiel
• Traitement médical débuté : Triatec, Bisoprolol, Lasilix,
Kardégic
!
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
1
/
40
100%