I. Polymenidi
A. Trombetti
S. Carballo
introduction
Les bisphosphonates sont largement utilisés dans la pratique
médicale. L’ostéonécrose des maxillaires associée aux bisphos-
phonates (ONBP) a été décrite pour la première fois en 2002.1
Onze ans plus tard, cette pathologie est toujours d’actualité et
de plus en plus médiatisée, notamment en raison de ses con-
séquences cliniques invalidantes et de la complexité du traite-
ment. Le but de cet article est de présenter quelques rappels sur les bisphospho-
nates, suivis d’une synthèse des données disponibles sur l’ONBP, en soulignant
les principaux points pour la pratique quotidienne de la médecine.
généralités concernant les bisphosphonates
Les bisphosphonates sont utilisés depuis plus de 30 ans dans le traitement de
l’ostéoporose et d’autres atteintes osseuses caractérisées par un remodelage ac-
céléré comme la maladie de Paget et les complications osseuses des cancers. Leur
bénéfice clinique dans la prévention des fractures ostéoporotiques a été démon-
tré par plusieurs études avec haut niveau de preuves (tableau 1).2 De nombreuses
études ont également démontré leur efficacité sur la réduction de la douleur et
de l’incidence des événements squelettiques (fracture, hypercalcémie) chez le
sujet avec cancer métastatique.3 Grâce à ces effets, les bisphosphonates sont des
outils précieux dans la pratique médicale quotidienne.
Les bisphosphonates inhibent la résorption osseuse via leur activité sur la
fonction des ostéoclastes. Ces analogues synthétiques du pyrophosphate inorga-
nique présentent une forte affinité pour l’os, où ils se lient fortement à l’hydroxy-
apatite (figure 1 et tableau 2). Ils sont ensuite ingérés par les ostéoclastes, dont ils
perturbent le métabolisme et inhibent l’action. Grâce à leur action antiostéoclas-
tique, les bisphosphonates réduisent le remodelage osseux, d’où un gain de den-
sité lié à un allongement de la période de minéralisation osseuse dite secondaire
et une diminution de la fragilité osseuse.4 En termes de pharmacocinétique, les
The risk of bisphosphonate-related
osteonecrosis of the jaw
Bisphosphonates are widely used in the
treatment of osteonecrosis and oncology re-
lated bone complications. Their use is highly
beneficial for the patient, but may be asso-
ciated with adverse effects. Osteonecrosis of
the jaw is an often cited complication of this
treatment, but is in practice rarely seen. Its pre-
valence is low in cases of osteoporosis but a
little higher in the oncological setting. Although
its pathophysiology is not completely eluci-
dated, certain risk factors have been identified
such as tooth extraction which often precedes
the affection. Management requires a multi-
disciplinary approach and a conservative treat-
ment is usually preferred. Dealing with this
rare condition requires identification of at risk
patients so as to apply preventative measures.
Rev Med Suisse 2014 ; 10 : 1930-4
Les bisphosphonates sont largement utilisés pour le traitement
de l’ostéoporose et des complications osseuses des cancers.
Les bénéfices associés à leur usage sont largement reconnus.
Certains risques sont toutefois liés à leur utilisation dont l’os-
téonécrose des maxillaires, une complication souvent média-
tisée, mais qui n’est rencontrée que rarement dans la pratique
médicale. Sa prévalence est faible en cas d’ostéoporose mais
plus importante dans le contexte oncologique. Le processus
physiopathologique n’est pas complètement élucidé mais cer-
tains facteurs de risque sont identifiés, dont l’extraction den-
taire qui précède souvent cette complication. La prise en charge
nécessite une approche multidisciplinaire et la plupart du
temps un traitement conservateur est privilégié. Face à cette
affection plutôt rare mais invalidante et difficile à traiter, il est
important d’identifier les patients à risque et d’appliquer des
mesures préventives.
Risque d’ostéonécrose
des maxillaires avec l’utilisation
des bisphosphonates
synthèse
1930 Revue Médicale Suisse
–
www.revmed.ch
–
15 octobre 2014
Drs Ioanna Polymenidi
et Sebastian Carballo
Service de médecine interne générale
Département de médecine interne,
réhabilitation et gériatrie
Dr Andrea Trombetti
Service des maladies osseuses
Département des spécialités
de médecine
HUG, 1211 Genève 14
Revue Médicale Suisse
–
www.revmed.ch
–
15 octobre 2014 0
38138
34_38_38138.indd 1 09.10.14 09:09

Revue Médicale Suisse
–
www.revmed.ch
–
15 octobre 2014 1931
bisphosphonates se caractérisent par une demi-vie squelet-
tique extrêmement longue, d’environ dix ans et qui varie
selon les composés.
ostéonécrose des maxillaires associée
aux bisphosphonates
Le premier cas d’ostéonécrose des maxillaires est rap-
porté en 1839 où l’on décrit une nécrose des maxillaires chez
les ouvriers qui manipulent du phosphore blanc dans les
manufactures d’allumettes
(phossy jaw)
. L’histoire se répète
pendant la période 1939-1945 avec l’utilisation du phos-
phore blanc dans l’industrie de l’armement qui entraîne un
grand nombre de nouveaux cas d’ostéonécrose des maxil-
laires.1 L’ostéonécrose des maxillaires est de retour en 2002,
quand Marx et Stern décrivent des lésions nécrotiques des
maxillaires chez les patients sous bisphosphonates.5 Malgré
une présentation similaire, la physiopathologie de ces deux
entités, la
phossy jaw
et l’ostéonécrose des maxillaires liée
à l’usage des bisphosphonates, est probablement très dif-
férente.
définition, présentation clinique
et épidémiologie
L’ONBP est définie par la présence d’os exposé au niveau
de la région maxillo-faciale qui persiste pendant minimum
huit semaines, chez les patients sous bisphosphonates, sans
antécédent de radiothérapie locale ni de métastases des
maxillaires. L’ONBP semble se manifester plus fréquemment
au niveau mandibulaire que maxillaire. Les patients présen-
tent une zone osseuse dénudée, de consistance dure, de
couleur brun jaunâtre et à surface rugueuse. L’atteinte peut
être asymptomatique ou se manifester par des douleurs, des
paresthésies dans le territoire du nerf alvéolaire inférieur,
une tuméfaction gingivale, osseuse et des sinus.6
L’ostéonécrose des maxillaires est rare et d’incidence
inconnue dans la population générale. Concernant son inci-
dence chez les patients sous bisphosphonates, les chiffres
sont variables surtout en raison du type d’études disponi-
bles (plutôt rétrospectives que prospectives) et de l’absence
d’une définition précise de cette pathologie jusqu’à récem-
ment.7 La grande majorité de la littérature concerne des
patients oncologiques sous hautes doses de bisphosphona-
tes intraveineux. L’incidence de l’ONBP dans cette popula-
tion est estimée entre 1 et 10%. On peut citer trois études
prospectives portant sur 5723 patients avec métastases os-
seuses sous zolédronate versus dénosumab, qui retrouvent
89 cas d’ONBP (incidence 1,6%), avec une incidence compa-
rable entre le dénosumab et le zolédronate (1,8 vs 1,2%).8
On constate ici que l’ostéonécrose des maxillaires est un
effet secondaire que les bisphosphonates partagent avec
le dénosumab, un traitement antirésorptif récent.
Concernant l’incidence de l’ONBP en cas d’ostéoporose,
il existe peu de données. Un registre allemand, qui com-
0 Revue Médicale Suisse
–
www.revmed.ch
–
15 octobre 2014
Fractures Fractures non Fracture
vertébrales vertébrales de la hanche
Alendronate A A A
Ibandronate A A* NA
Risédronate A A A
Zolédronate A A A
Calcitonine A NA NA
Calcitriol A NA NA
Raloxifène A NA NA
Ranélate de strontium A A A*
Dénosumab A A A
Tériparatide A A NA
Traitement hormonal A A A
substitutif
(Adapté de l’Association suisse contre l’ostéoporose, recommandations
2010).1
A, B : degré d’évidence ; NA : non évalué de façon adéquate.
* Uniquement chez des sous-groupes de patients (analyse post-
hoc).
Tableau 1. Prévention des fractures ostéoporotiques
Tableau 2. Génération et puissance relative des
bisphosphonates
Molécules Noms Voies Puissances
commerciaux d’administration
Bisphosphonates 1re génération : non aminés
Etidronate Didronel Orale 1
Clodronate Bonefos Orale, IV 10
Tiludronate Skelid Orale 10
Aminobisphosphonates 2e génération
Pamidronate Arédia IV 100
Alendronate Fosamax Orale 1000
Fosavance Orale
Aminobisphosphonates 3e génération
Risédronate Actonel Orale 5000
Ibandronate Bondronat IV 10 000
Bonviva
Zolédronate Zometa IV 20 000
Aclasta IV
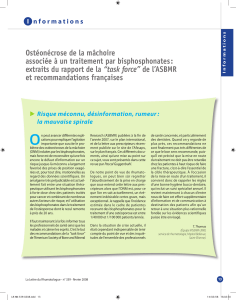
Figure 1. Bisphosphonates
La chaîne R2 est celle qui définit l’activité antiostéoclastique des bisphos-
phonates. Sa modification a engendré trois générations de bisphosphonates,
de puissance croissante mais au prix d’un plus grand nombre d’effets in-
désirables. En ajoutant un atome d’azote à ce groupe R2, on obtient les
aminobisphosphonates.
Pyrophosphate Bisphosphonate
34_38_38138.indd 2 09.10.14 09:09

Revue Médicale Suisse
–
www.revmed.ch
–
15 octobre 2014 0
prend plus que 300 rapports de cas d’ONBP, retrouve seu-
lement trois patients sous bisphosphonates per os.9 Selon
les firmes pharmaceutiques, qui prennent en considéra-
tion les déclarations spontanées d’ONBP des patients, on
retrouve une incidence d’un événement par 100 000 person-
nes/année d’exposition aux bisphosphonates oraux.10 Des
données australiennes révèlent une incidence de 1/10 000.11
L’utilisation des bisphosphonates intraveineux pour l’os-
téoporose étant récente, on dispose à l’heure actuelle de
peu de données sur l’incidence d’ONBP sous bisphospho-
nates IV aux doses approuvées pour l’ostéoporose par rap-
port au traitement oral. Des données issues d’enquêtes
réalisées par des équipes de chirurgie maxillo-faciale rap-
por tent toutefois des fréquences plus élevées, de l’ordre
de 0,001 à 0,1%.12,13 Des études épidémiologiques plus ré-
cen tes rapportent une incidence de l’ordre de 0,02%.14
physiopathologie et facteurs de risque
Le processus physiopathologique de l’ONBP n’est tou-
jours pas élucidé. Un des mécanismes proposés est la dimi-
nution du remodelage osseux sur le long terme. L’hypothèse
est qu’un traitement prolongé rend l’os adynamique, avec
diminution du flux sanguin, nécrose des cellules osseuses
et apoptose. Pour le moment, il n’y a pas suffisamment de
données dans la littérature pour soutenir fermement cette
hypothèse.7
Le facteur précipitant fréquemment retrouvé dans toutes
les publications est un traumatisme préalable de la mu-
queuse orale. Dans les trois études prospectives de Saad,
une extraction dentaire précède l’ONBP dans 62% des cas.8
Hormis l’extraction dentaire, il existe d’autres facteurs de
risque locaux : procédures chirurgicales exposant l’os des
mâchoires, érosions liées aux prothèses dentaires, parodon-
tite, abcès et caries.
L’infection est une composante classique de l’ONBP. La
plupart des analyses histopathologiques révèlent un état
inflammatoire et retrouvent le germe
Actinomyces
. On ne sait
pas si l’infection précède l’ONBP ou si les tissus nécroti-
ques se surinfectent secondairement. L’expérience clini-
que montre une amélioration des lésions ostéonécrotiques
après un traitement antibiotique, mais il n’y a pas d’étude
contrôlée qui évalue l’efficacité d’une antibiothérapie ciblée
sur l’actinomycose.7
Les corticoïdes et le diabète peuvent théoriquement fa-
voriser une ONBP, notamment en raison du ralentissement
de la cicatrisation et de l’immunosuppression.7 Toutefois,
les études prospectives menées par Saad et coll. et l’étude
rétrospective de Hoff et coll. ne retrouvent pas d’associa-
tion statistiquement significative entre les corticoïdes et
l’ONBP
.8,15 Concernant le diabète, une étude, réalisée entre
2004 et 2006 chez 31 patients ayant une ONBP, retrouve dix-
huit personnes diabétiques ou intolérantes au glucose, soit
58%.16
Concernant le rôle de l’angiogenèse, il existe des études
in vitro ou sur des modèles animaux qui montrent une inhi-
bition de l’angiogenèse par les bisphosphonates.7 Dans une
étude rétrospective, l’usage concomitant de bévacizumab,
de sunitinib ou de sorafénib avec les bisphosphonates
augmente la fréquence de l’ONBP à 16% (versus 1,1% pour
les bisphosphonates seuls).17 Les études prospectives de
Saad et coll. ne retrouvent pas d’association entre l’ONBP
et le traitement antiangiogénique.8
Un facteur de risque important est la forme du traitement :
la dose, la puissance de la molécule et la durée du traite-
ment sont en corrélation avec l’apparition de l’ONBP. Une
revue de la littérature sur l’ONBP entre 2003 et 2008 met en
évidence les éléments suivants.18
• Chez les patients ostéoporotiques sous bisphosphonates
oraux (alendronate et risédronate), on retrouve 103 cas
d’ONBP avec une durée moyenne du traitement jusqu’à
l’apparition de l’ONBP de 4,6 ans et de minimum 3 ans, avec
une dose cumulative de 13 870 mg.
• Chez les patients sous pamidronate, dont l’administration
est intraveineuse, on retrouve 165 cas d’ONBP, avec une
durée moyenne du traitement jusqu’à l’apparition de l’ONBP
de 2,8 ans et de minimum 1,5 an, avec une dose cumulative
de 2217 mg.
• Chez les patients sous zolédronate, dont l’administration
est également intraveineuse, on retrouve 388 cas d’ONBP,
avec une durée moyenne du traitement jusqu’à l’apparition
de l’ONBP de 1,8 an et de minimum dix mois, avec une
dose cumulative de 49 mg.
Le type de cancer a pu être associé à l’ONBP. L’inciden-
ce d’ONBP paraît augmentée (2-11%) chez les patients souf-
frant d’un myélome multiple, probablement en raison de
l’atteinte des maxillaires et d’une inhibition marquée de la
formation osseuse, alors qu’elle est rarement impliquée
dans les métastases osseuses d’autres cancers.19 L’étude
de Hoff et coll. retrouve une association entre l’ONBP et la
positivité des récepteurs aux œstrogènes chez les patientes
souffrant d’un cancer du sein.15 Cette observation serait
plutôt expliquée par un meilleur pronostic de la maladie
associé à une survie plus longue, une exposition aux bis-
phosphonates plus longue et des doses cumulatives plus
importantes.
Le tabac et l’alcool peuvent favoriser une ONBP mais pour
le moment les évidences sont faibles.20 Une toxicité directe
des bisphosphonates sur les muqueuses est également
évoquée par certains auteurs, avec à la clé de ce mécanisme
une inhibition de la cicatrisation de la paroi des cellules des
kératinocytes.21,22
En conclusion, l’hypothèse qui prévaut actuellement est
une exposition osseuse aux bactéries de la cavité buccale.
Il se développe alors une nécrose osseuse, mais le séques-
tre osseux ne peut être résorbé ou remodelé du fait du
mécanisme d’action des bisphosphonates (de même que
celui du dénosumab). L’effet antiangiogénique des bisphos-
phonates est un facteur aggravant.7
pourquoi l’os maxillaire ?
La mâchoire a une vascularisation et un taux de renou-
vellement cellulaire plus importants que d’autres os, par la
présence des dents qui nécessitent un remodelage fré-
quent. Ces caractéristiques conduisent à une concentration
en bisphosphonates supérieure à celle des autres os.23 Par
ailleurs, la cavité orale est un environnement polybactérien,
qui subit des microtraumatismes intenses. L’os des maxil-
laires est séparé de cet environnement seulement par une
1932 Revue Médicale Suisse
–
www.revmed.ch
–
15 octobre 2014
34_38_38138.indd 3 09.10.14 09:09

Revue Médicale Suisse
–
www.revmed.ch
–
15 octobre 2014 1933
muqueuse fine et le périoste, une barrière très fragile.23 En
2006, les premiers cas d’ONBP en dehors de la région orale
ont été décrits, favorisant l’hypothèse qu’il s’agit d’une com-
plication osseuse systémique.24,25
comment en faire le diagnostic
et comment traiter ?
Le diagnostic est posé par l’anamnèse et l’examen cli-
nique. Un orthopantomogramme est utile notamment pour
le suivi, mais un CT ou une IRM sont préférables pour dé-
terminer l’étendue des nécroses osseuses et les modifica-
tions inflammatoires de l’os et des tissus mous. Le fait que
les bisphosphonates soient prescrits par le médecin géné-
raliste, l’oncologue ou un autre spécialiste, mais que la né-
crose apparaisse dans la zone de traitement du médecin
dentiste, complique l’approche de cette maladie.26
L’AAOMS (American Association of Oral and Maxillofacial
Surgeons) propose une stratégie thérapeutique en fonction
du stade de la maladie (tableau 3).20 L’approche conserva-
trice dans la mesure du possible est le traitement de choix.
Dans les études prospectives de Saad et coll., parmi les
89 cas d’ONBP, 54% des patients ont été traités de manière
conservative et 41% ont été opérés a minima.8 Une résec-
tion de l’os affecté a été effectuée chez seulement quatre
patients. Une résolution complète de l’ONBP a été obser-
vée chez 32 pa tients, donc le risque de chronicité est très
important. Quel ques données existent sur l’utilisation de
la tériparatide, une molécule qui comprend les premiers
34 acides aminés de l’hormone parathyroïdienne (PTH), et
qui a des effets anabolisants sur l’os.27,28 Ce médicament a
surtout été étudié dans le contexte de l’ostéoporose.
arrêt thérapeutique (drug holiday) ?20,29
L’arrêt des bisphosphonates n’assure pas la guérison des
nécroses en raison de leur longue demi-vie squelettique
(environ dix ans). Cependant, l’arrêt prolongé pourrait sta-
biliser la progression des lésions et réduire le risque d’ap-
parition de nouveaux sites d’exposition osseuse. En revan-
che, il y a un risque de progression des métastases et des
douleurs osseuses. La décision de l’arrêt du traitement né-
cessite donc une évaluation multidisciplinaire.
prévention
Face à la résistance de l’ONBP aux stratégies thérapeuti-
ques disponibles, la prévention a une place clé. L’«American
Society for Bone and Mineral Research» a proposé des me-
sures préventives en 2007, mesures qui sont résumées dans
le tableau 4. Une étude effectuée par Dimopoulos et coll.
suggèrent que l’application des mesures préventives dimi-
nue le risque d’ONBP.30
adaptation du schéma d’administration
des bisphosphonates
En prévention de l’ONBP, il semble envisageable d’appli-
quer un schéma réduit permettant à la fois de minimiser le
risque d’événements squelettiques et celui d’ONBP. L’étude
rétrospective de Corso et coll. a comparé le schéma stan-
dard de zolédronate versus un schéma réduit (une injection
par mois pendant un an et puis tous les trois mois) dans
0 Revue Médicale Suisse
–
www.revmed.ch
–
15 octobre 2014
Stades de l’ONBP Descriptions Traitements
A risque Patient exposé aux bisphosphonates sans évidence d’os nécrotique Pas de traitement, éducation du patient
Stade 0 Pas d’évidence clinique d’os nécrotique mais présence de Antalgie, antibiothérapie
symptômes et de signes cliniques aspécifiques
Stade I Lésions asymptomatiques avec exposition osseuse sans signe Asepsie locale, suivi rapproché
infectieux
Stade II Os exposé, douleur, infection et tuméfaction Antibiothérapie orale, rinçage buccal antibiotique, antalgie,
débridement superficiel
Stade III Os exposé, douleur, inflammation, atteinte des sinus maxillaires, Antibiothérapie, rinçage buccal antibiotique, antalgie,
fistules cutanées, fractures pathologiques débridement chirurgical et résection pour contrôler
l’infection et la douleur
Tableau 3. Classification et stades de l’ostéonécrose des maxillaires associée aux bisphosphonates (ONBP)
(Adapté de réf.32).
Tableau 4. Utilisation des bisphosphonates en
pratique
Recommandations générales
• Communication entre le médecin généraliste, le dentiste et le patient.
Encourager le patient à signaler la prise de bisphosphonates
• Informer le patient des risques et des bénéfices des bisphosphonates
• Encourager une bonne hygiène dentaire
• Education des médecins et des patients sur l’ostéonécrose des maxil-
laires associée aux bisphosphonates (ONBP)
Avant l’introduction des bisphosphonates pour l’ostéoporose
• Informer le patient du risque d’ONBP (entre 1/10 000 et 1/100 000)
• Un contrôle dentaire avant le début du traitement n’est pas nécessaire
car le risque est faible et surtout associé à la durée du traitement
• Encourager un suivi dentaire de routine et une bonne hygiène dentaire
• Si traitement L 3 ans, prendre des précautions supplémentaires : éviter
les interventions dentaires, si l’intervention est nécessaire, évaluer
l’arrêt transitoire du traitement
Avant l’introduction des bisphosphonates IV aux doses
oncologiques
• Informer le patient du risque d’ONBP (environ 1%)
• Contrôle dentaire avant le début du traitement, à répéter tous les six
à douze mois
• Si le traitement par bisphosphonates peut attendre : effectuer toute
intervention dentaire avant, introduire le traitement après une guérison
buccale complète
• Eviter toute intervention dentaire qui n’est pas absolument nécessaire
34_38_38138.indd 4 09.10.14 09:09

Revue Médicale Suisse
–
www.revmed.ch
–
15 octobre 2014 0
son indication oncologique.31 On constate que l’incidence
des complications osseuses est similaire mais le risque
d’ONBP est huit fois plus bas avec le schéma réduit.
conclusions
L’ONBP est une complication rare en cas d’ostéoporose
mais plus fréquente en présence d’atteinte oncologique.
Dans la grande majorité des cas, elle survient après une
extraction dentaire. C’est un effet secondaire que les bis-
phosphonates partagent avec le dénosumab. La préven-
tion occupe une place majeure : il est important d’identifier
les patients à risque et d’appliquer des stratégies de réduc-
tion de risque. L’information des patients quant aux risques
d’ONBP ne doit pas être un frein à la prescription des bis-
phosphonates ni à l’observance de ce traitement. La préven-
tion et le traitement de l’ONBP nécessitent une prise en
charge multidisciplinaire entre le médecin généraliste, l’on-
cologue, le dentiste et le chirurgien maxillo-facial. La recher-
che doit encore apporter des réponses quant à la physio-
pathologie, le traitement et l’efficacité des mesures préven-
tives.
1934 Revue Médicale Suisse
–
www.revmed.ch
–
15 octobre 2014
Les auteurs n’ont déclaré aucun conflit d’intérêts en relation avec
cet article.
Implications pratiques
L’ostéonécrose des maxillaires associée aux bisphosphonates
est rare lorsque l’indication du traitement est l’ostéoporose,
beaucoup plus fréquente (jusqu’à 1%) lors de l’utilisation chez
les patients oncologiques
Il s’agit d’un effet secondaire que les bisphosphonates par-
tagent avec le dénosumab
Le facteur de risque le plus important est un traumatisme
préalable de la muqueuse orale
Le traitement dépend du stade de la maladie. Une traite-
ment conservateur est privilégié dans la plupart des cas
La prévention et l’approche multidisciplinaire sont la clé de
la prise en charge
>
>
>
>
>
1 Carrel JP, Seeman A, Lysitsa L. Phosphore et bis-
phosphonates : ou quand on oublie les leçons du passé.
Med Buccale Chir Buccale 2006;2006:8-14.
2 Association suisse contre l’ostéoporose. Ostéopo-
rose : prévention, diagnostic, traitement. Recomman da-
tions. 2010.
3 Ross JR, Saunders Y, Edmonds PM, et al. Systematic
review of role of bisphosphonates on skeletal morbi-
dity in metastatic cancer. BMJ 2003;327:469.
4 Desmeules J. Bisphosphonates au long cours : sécu-
rité remise en question ? Pharma-Flash 2009;2009:1-4.
5 Marx RE, Stern D. Oral and maxillofacial pathology :
A rationale for treatment. Hanover Park 2002.
6 Gratz K, Zwahlen R. Ostéonécrose maxillaire as-
sociée aux bisphosphonates. Rev Mens Suisse Odonto-
stomatol 2008;2008:119-23.
7 ** Rizzoli R, Burlet N, Cahall D, et al. Osteonecro-
sis of the jaw and bisphosphonate treatment for osteo-
porosis. Bone 2008;42:841-7.
8 ** Saad F, Brown JE, Van Poznak C, et al. Inciden ce,
risk factors, and outcomes of osteonecrosis of the jaw :
Integrated analysis from three blinded active-control-
led phase III trials in cancer patients with bone meta-
stases. Ann Oncol 2012;23:1341-7.
9 Felsenberg D. Kiefernekrosen nach hoch dosierter
Bisphosphonattherapie. Dtsch Arztebl 2006;2006:3078-
80.
10 Bilezikian JP. Osteonecrosis of the jaw – do bisphos-
phonates pose a risk ? N Engl J Med 2006;355:2278-81.
11 Mavrokokki T, Cheng A, Stein B, Goss A. Nature
and frequency of bisphosphonate-associated osteone-
crosis of the jaws in Australia. J Oral Maxillofac Surg
2007;65:415-23.
12 Khan AA, Rios LP, Sandor GK, et al. Bisphospho-
nate-associated osteonecrosis of the jaw in Ontario : A
survey of oral and maxillofacial surgeons. J Rheumatol
2011;38:1396-402.
13 Lo JC, O’Ryan FS, Gordon NP, et al. Prevalence of
osteonecrosis of the jaw in patients with oral bisphos-
phonate exposure. J Oral Maxillofac Surg 2010;68:243-
53.
14 * Solomon DH, Mercer E, Woo SB, et al. Defining
the epidemiology of bisphosphonate-associated osteo-
necrosis of the jaw : Prior work and current challenges.
Osteoporos Int 2013;24:237-44.
15 Hoff AO, Toth BB, Altundag K, et al. Frequency
and risk factors associated with osteonecrosis of the jaw
in cancer patients treated with intravenous bisphospho-
nates. J Bone Miner Res 2008;23:826-36.
16 Khamaisi M, Regev E, Yarom N, et al. Possible as-
sociation between diabetes and bisphosphonate-related
jaw osteonecrosis. J Clin Endocrinol Metab 2007;92:
1172-5.
17 Christodoulou C, Pervena A, Klouvas G, et al.
Combination of bisphosphonates and antiangiogenic
factors induces osteonecrosis of the jaw more fre-
quently than bisphosphonates alone. Oncology 2009;
76:209-11.
18 Palaska PK, Cartsos V, Zavras AI. Bisphosphonates
and time to osteonecrosis development. Oncologist
2009;14:1154-66.
19 Delibasi T, Altundag K, Kanlioglu Y. Why osteone-
crosis of the jaw after bisphosphonates treatment is
more frequent in multiple myeloma than in solid tumors.
J Oral Maxillofac Surg 2006;64:995-6.
20 * Ruggiero SL, Dodson TB, Assael LA, et al. Ame-
rican Association of Oral and Maxillofacial Surgeons
position paper on bisphosphonate-related osteonecro-
sis of the jaws – 2009 update. J Oral Maxillofac Surg
2009;67:2-12.
21 Landesberg R, Cozin M, Cremers S, et al. Inhibition
of oral mucosal cell wound healing by bisphosphonates.
J Oral Maxillofac Surg 2008;66:839-47.
22 Reid IR, Bolland MJ, Grey AB. Is bisphosphonate-
associated osteonecrosis of the jaw caused by soft tissue
toxicity ? Bone 2007;41:318-20.
23 Madrid C, Jaques B, Bouferrache K, Broome M.
Management of complications of bisphosphonates in
oncology patients : Jaw osteonecrosis. Rev Med Suisse
2007;3:1322, 1324-6, 1329-31.
24 Longo R, Castellana MA, Gasparini G. Bisphospho-
nate-related osteonecrosis of the jaw and left thumb. J
Clin Oncol 2009;27:e242-3.
25 Polizzotto MN, Cousins V, Schwarer AP. Bisphos-
phonate-associated osteonecrosis of the auditory canal.
Br J Haematol 2006;132:114.
26 Dannemann C, Gratz K, Zwahlen R. Ostéonécrose
maxillaire associée aux bisphosphonates. Rev Mens
Suisse Odontostomatol 2008;2008:119-23.
27 Cheung A, Seeman E. Teriparatide therapy for
alendronate-associated osteonecrosis of the jaw. N Engl
J Med 2010;363:2473-4.
28 Lau AN, Adachi JD. Resolution of osteonecrosis of
the jaw after teriparatide (recombinant human PTH-
(1-34)) therapy. J Rheumatol 2009;36:1835-7.
29 * Khosla S, Burr D, Cauley J, et al. Bisphosphonate-
associated osteonecrosis of the jaw : Report of a task
force of the American Society for Bone and Mineral
Research. J Bone Miner Res 2007;22:1479-91.
30 Dimopoulos MA, Kastritis E, Bamia C, et al. Reduc-
tion of osteonecrosis of the jaw (ONJ) after implementa-
tion of preventive measures in patients with multiple
myeloma treated with zoledronic acid. Ann Oncol 2009;
20:117-20.
31 Corso A, Varettoni M, Zappasodi P, et al. A dif-
ferent schedule of zoledronic acid can reduce the risk of
the osteonecrosis of the jaw in patients with multiple
myeloma. Leukemia 2007;21:1545-8.
32 Vescovi P, Nammour S. Bisphosphonate-Related
Osteonecrosis of the Jaw (BRONJ) therapy. A critical
review. Minerva Stomatol 2010;59:181-203, 204-13.
* à lire
** à lire absolument
Bibliographie
34_38_38138.indd 5 09.10.14 09:09
1
/
5
100%