Amylose AA?

NOUVELLES CIBLES THERAPEUTIQUES DANS
LES MALADIES AUTOINFLAMMATOIRES
Dr Sophie Georgin-Lavialle
Centre de référence des amyloses d’origine inflammatoire et de la fièvre méditerranéenne familiale, Hôpital Tenon, Paris
Colloque du CEREMAI, Montpellier, le Vendredi 16 Octobre 2015

PLAN
•Traitement en fonction du mécanisme physiopathologique
•=> nouvelles thérapies ciblées
•Approche par type cellulaire
•Déficit immunitaire et MAI
•Amylose AA

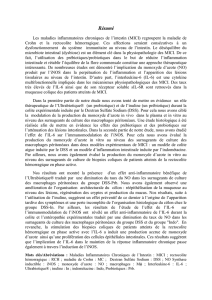
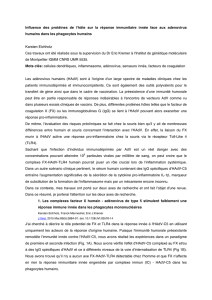
Inflammasome
Caspase active
IL-18
IL-1 b
Adapted from Holzinger, Nat Rev Rheum, 2015
Noyau
R.E
ProIL-1 b
ProIL-18
IL-6, TNFa, DAMPS
IL-6
TNFa
S100
HMGB1
IL-18 BP
IL-1RA
IL-36RA
ROS
INFLAMMASOMOPATHIES: mutations
gain de fonction des inflammasommes:
secretion d’Il1b et IL18
ATP
Stress RE
INTERFERONOPATHIES: augmentation
de l’expression du gene de l’INF et de
l’inflammation
TNFR
IL-6 R
IL-1 R
PAMPs/DAMPs
Monocyte
STRESS DU RETICULUM ENDOPLASMIQUE:
Défaut de repliement des protéines ou défaut de
modifications post translationnelles: augmentation du
stress RE =>Secretion accrue de ROS => production Il1b
Déséquilibre des antagonistes endogènes:
Mutations IL1RN, IL36RN

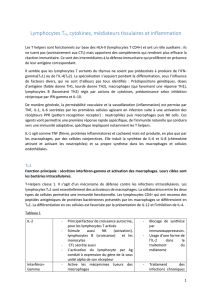
Inflammasome
Caspase active
IL-18
IL-1 b
Holzinger, Nat Rev Rheum, 2015
Noyau
R.E
ProIL-1 b
ProIL-18
IL-6, TNFa, DAMPS
IL-6
TNFa
S100
HMGB1
IL-18 BP
IL-1RA
IL-36RA
ROS
INFLAMMASOMOPATHIES: mutations
gain de function des inflammasommes:
secretion d’Il1b et IL18
ATP
Stress RE
TNFR
IL-6 R
IL-1 R
PAMPs/DAMPs
Monocyte

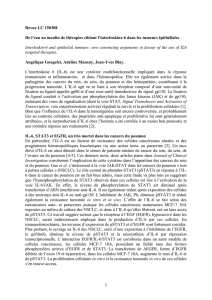
Inflammasome
Caspase active
IL-18
IL-1 b
Holzinger, Nat Rev Rheum, 2015
Noyau
R.E
ProIL-1 b
ProIL-18
IL-6, TNFa, DAMPS
IL-6
TNFa
S100
HMGB1
IL-18 BP
IL-1RA
IL-36RA
ROS
INFLAMMASOMOPATHIES: mutations
gain de function des inflammasommes:
secretion d’Il1b et IL18
ATP
Stress RE
TNFR
IL-6 R
IL-1 R
PAMPs/DAMPs
Monocyte
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
1
/
34
100%