Dysthyroïdie

Dysthyroïdie
Dr JJaafar
Dr
J
Jaafar
Serviced’endocrinologie
HUG
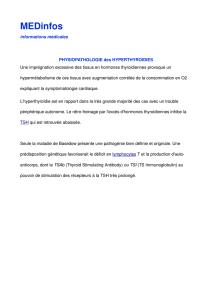
Histolo
g
ie
g
Réseaucapillaireautourdesfollicules
thyroïdiens.MottaP.Anatomiemicroscopique.
Editionfrançaise,PICCIN1988

L
’
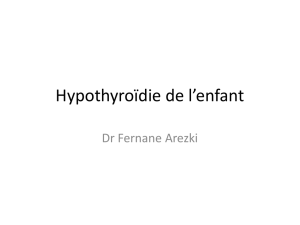
iode substrat des hormones thyroïdiennes
L iode
,
substrat
des
hormones
thyroïdiennes
Apportsrecommandés:
Adulte 150
mcg
/j
Adulte
150
mcg
/j
.
Femmeenceinte200mcg/j.
Synthesisofthyroidhormones
Cohen‐Lehman,J.etal. (2009)Nat.Rev.Endocrinol.
Physiologie
Hormones thyroïdiennes
Hormones
thyroïdiennes
SécrétionSécrétionthyroïdienne:thyroïdienne:
•• 9090%deT4%deT4
•• 1010%de%deT3(hormoneactive)T3(hormoneactive)
ConversionConversionpériphériquedeT4enT3(périphériquedeT4enT3(déiodinasesdéiodinases))
DemiDemi‐‐vie:vie:
––
T4: 1semaineT4: 1semaine
––
T4:
1
semaine
T4:
1
semaine
–– T3:1.5jourT3:1.5jour
T4/T3totale=T4/T3libre+T4/T3liée.T4/T3totale=T4/T3libre+T4/T3liée.
Liaison:(TBG,Liaison:(TBG,TransthyrétineTransthyrétine,Albumine),Albumine)
FractionlibredeT3=0.4%FractionlibredeT3=0.4%
FractionlibredeT4=0.04%FractionlibredeT4=0.04%

Th
y
réostimuline/TSH
y
h
Demi‐vie1
h
Dépistage,etsuivi
Variationenfonctionde:
•
L
’
âge
•
Lâge
•L’ethnie
Le phénomène Wolff
Chaikoff
Le
phénomène
Wolff
‐
Chaikoff
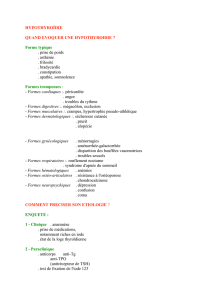
Effets des hormones thyroïdiennes
Effets
des
hormones
thyroïdiennes
SchmaltzC.Adv NeonatalCare.2012
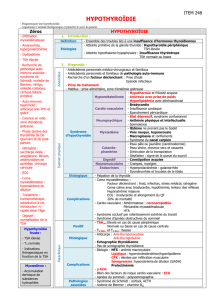
L’hypothyroïdie

Hypothyroïdie
prévalence
Colorado
thyroid
disease
prevalence
study
arch
intern
Med 2000
Feb
28;160(4):526
34
Colorado
thyroid
disease
prevalence
study
,
arch
intern
Med
.
2000
Feb
28;160(4):526
‐
34
.
Clinique
Clinique
Frilosité
Peausèche
Cheveux/ongles cassants
Cheveux/ongles
cassants
Bradycardie
Fatigue,ralentissement
psychomoteur,dépression
Prisedepoids
Constipation
Œdèmes
ªréflexes
Troubles cycle
Troubles
cycle
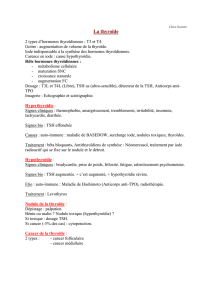
PercentageofEuthyroid,Subclinicaland
HypothyroidPatientsReportingSymptoms
60%euthyroid
have≥1symptom
15%
≥4 t
15%
≥
4
symp
t
oms
R5.Clinicalscoringsystemsshouldnotbeusedtodiagnose
hypothyroidism. Grade A, BEL 1
Canaris et al.
hypothyroidism.
Grade
A,
BEL
1
Prévalence des AC
Prévalence
des
AC
TRAb
AC ti
TPO
AC ti T
TRAb
AC
an
ti
TPO
AC
an
ti
T
g
Population générale 0% 5‐20% 8‐27%
Basedow
80
‐
95%
50
‐
70%
50
‐
80%
Basedow
80
95%
50
70%
50
80%
Hashimoto 10‐20% 80‐90% 90‐100%
Thyroïdite silencieuse 0% 25% 60%
AF+pourHashimoto 0% 30‐50% 30‐50%
Diabètedetype10% 30‐40% 30‐40%

H
yp
oth
y
roïdie
yp y
Hypothyroïdie
subclinique
Hypothyroïdie
franche
Hypothyroïdie
centrale
subclinique
franche
centrale
TSH ↑↑Normaleà↓
T4l « Normale » ↓↓
Fréquence 5‐10% Rare
HypothyroïdiecentraleHypothyroïdiecentrale
‐TSHpeut‐être«normale»(maisinadaptéevuªT4)
ÎsisuspicionhypoT centrale:demanderT4libre!
Etiologies
Etiologies
hïdi ii(9%)
Th ïdi hi
i ( Hhi )
Hypot
h
yro
ïdi
epr
i
ma
i
re
(
>
9
5
%)
Th
yro
ïdi
tec
h
ron
i
queauto‐
i
mmune
(
H
as
hi
moto
)
Thyroïdite(silencieuse,postpartum,DeQuervain)
Iatrogène:
A
p
rèsth
y
roïdectomie
,
radio‐iode
,
irradiation
py,
,
cervicale.
Médicamenteux:amiodarone ,lithium,
antithyroïdiens,…)
Sh idé (ditdtt)
S
urc
h
arge
i
o
dé
es
(
pro
d
u
it
d
econ
t
ras
t
e
)
Maladieinfiltratives (Riedel,sarcoidiose,amyloidose…)
Hypothyroïdie secondaire (<5%)
Macroadénome
hypophysaire craniopharyngiome
Hypothyroïdie
secondaire
(
<5%)
Macroadénome
hypophysaire
,
craniopharyngiome
,
méningiome,tumeursellaire)
Aprèschirurgieouradiothérapiehypophysaire
Hypophysite
Sarcoïdose,histiocytose,hémochromatose
SyndromedeSheehan
Infection(TBC,toxoplasmose)
Bilan d
’
une hypothyroïdie
Bilan
d une
hypothyroïdie
•Quefaire:
–
Ré
p
éterTSH?
p
–T4letT3?
Anticorps anti
TPO anti Tg
TRAb
?
–
Anticorps
anti
‐
TPO
,
anti
Tg
,
TRAb
?
–Thyroglobuline?
–
Imagerie?
–
Autres?
Biland’unehypothyroïdie:contrôlerlaTSH
Lesdysthyroïdies transitoires:
subaiguëdeDeQuervain
•probablecausevirale(rechercherviroseàl’anamnèse)
•
thyroïde
douloureuse !
thyroïde
douloureuse
!
•Tt:ββ,AINS+/‐glucocorticoïdes
dupost‐partum
Pas d’ATS !
•auto‐immune
•fréquente,maissilencieuse
•dansles6moispost‐partum
silencieuse
id
à
Parfois substitution
•
id
em
à
post‐partum
•Tt:symptomatique(ββ)
médics:
amiodarone lithium interféron
alpha
‐
médics:
amiodarone
,
lithium
,
interféron
‐
alpha
 6
7
8
9
10
11
12
13
6
7
8
9
10
11
12
13
1
/
13
100%