HER2 et cancers du sein HER2 and breast cancers »

Correspondances en Onco-Théranostic - Vol. I - n° 2 - avril-mai-juin 2012
57
HER2 et cancers du sein
HER2 et cancers du sein
HER2 and breast cancers
Anne Vincent-Salomon*
* Département de patho-
logie, Institut Curie, Paris.
RÉSUMÉ
Summary
»
La détermination du statut de HER2 est indispensable au moment
diagnostique initial des cancers infi ltrants du sein afi n de défi nir
la classe moléculaire de la tumeur et les possibilités d’utilisation
de thérapie ciblée anti-HER2. Le statut de HER2 est déterminé par
immunohistochimie en première intention et par hybridation in
situ pour vérifi er les scores 2+. Les taux de surexpression (score 3+)
de HER2 sont différents en fonction du type histologique, du
grade, du stade de la tumeur et varient de 9 à 30 %. La fi abilité
de la détermination requiert un contrôle de qualité externe et
interne strict avec, en particulier, l’utilisation de témoins externes
de manipulation au nombre de copies du gène HER2 connues.
Les tumeurs anti-HER2 sont une entité distincte des autres types
moléculaires mais forment un groupe hétérogène en fonction du
statut des récepteurs hormonaux, du niveau élevé ou faible de
l’amplifi cation de HER2, des anomalies chromosomiques associées à
cette amplifi cation et de la nature du stroma lymphoïde ou non. Les
critères de réponse aux thérapies ciblées anti-HER2 sont de mieux
en mieux connus (niveau d’amplifi cation de HER2, mutations des
autres gènes de la voie de transmission du signal intracellulaire tels
que PI3KCA ou la perte de PTEN). Les données issues du séquençage
parallèle massif apporteront un éclairage encore plus fin des
paramètres déterminant la sensibilité des tumeurs aux anti-HER2
et permettront d’optimiser les combinaisons de thérapies ciblées
afi n d’augmenter leur effi cacité.
Mots-clés : HER2 – Immunohistochimie – Cancers du sein – Taux de
surexpression – Résistance aux anti-HER2.
HER2 status determination is mandatory for all invasive
breast carcinomas at initial diagnosis in order to determine
their molecular class, and the indication of anti HER2
targeted therapy. This status is determined up-front by
immunohistochemistry followed by in situ hybridization
for 2+ scores. HER2 over expression rates vary from 9 to 30%,
these diff erences being related to histological types, grade
and stage. The accuracy of this determination relies on the
use of internal and external quality controls as defi ned by
international recommendations. The use of external controls
composed of tumor samples with a known number of HER2
gene copies is required. HER2 amplifi ed breast carcinomas
represent a distinct entity from other molecular subtypes
but encompass several sub-groups defi ned by the hormonal
receptor status, the level of HER2 amplification and the
presence of a lymphoid stroma. Predictive parameters of
response to anti HER2 therapies have been defi ned during
the past ten years such as level of HER2 amplification,
PI3KCA mutations or PTEN loss. Data from next generation
sequencing should refi ne predictive markers of anti HER2
sensitivity and help to determine the optimal combinations
of targeted therapies in the next future.
Keywords: HER2 – Breast cancers – Immunohistochemistry –
Rates of positivity – Resistance to anti-HER2.
L’
existence d’une amplification récurrente de
l’oncogène HER2 dans les cancers du sein
a été découverte par Dennis Slamon et al.
en 1987 (1). La survenue de l’amplification de HER2
était alors associée à une évolution défavorable de
la maladie liée entre autres à une augmentation
des capacités de prolifération et de croissance des
cellules tumorales, conséquences de l’amplification
de l’oncogène.
Quinze ans après cette découverte, une thérapie
ciblée anti-HER2 était mise à la disposition des
oncologues : le trastuzumab. Grâce à cette théra-
pie, le pronostic des patientes atteintes d’un can-
cer HER2 amplifié s’est considérablement amélioré.
Cette possibilité thérapeutique nécessitait donc une
détermination précise du statut HER2 des carcinomes
mammaires au diagnostic. Ainsi, en parallèle de la
description de leur statut hormonal, la définition du
statut de HER2 venait compléter leur caractérisation
et a donc mis en lumière l’existence des tumeurs triple
négatives.
En 10 ans d’utilisation du trastuzumab, du fait aussi de
l’arrivée d’autres molécules ciblant la voie HER2 et d’une
meilleure connaissance de la diversité biologique des

Correspondances en Onco-Théranostic - Vol. I - n° 2 - avril-mai-juin 2012
58
dossier thématique
Marqueurs prédictifs
de sensibilité et
de résistance aux anti-HER
carcinomes mammaires, nous avons pu approfondir nos
connaissances sur les carcinomes HER2 amplifi és et les
paramètres conditionnant la réponse aux traitements
anti-HER2, ainsi que sur les prérequis indispensables à la
caractérisation du statut de HER2 en pratique clinique.
L’oncogène HER2
L’oncogène HER2 (c-erbb2/neu) est localisé sur le bras
long du chromosome 17 (en 17q1.2 ; de 35,109 à
35,138 Mb). Ce gène est un membre de la famille du
récepteur à l’Epidermal Growth Factor (EGFR), famille
de récepteurs transmembranaires à activité tyrosine
kinase. Le gène HER2 code pour un récepteur qui n’a
pas de domaine de liaison à un ligand. Toutefois, HER2
forme des hétérodimères avec les autres membres
de la famille de l’EGFR, favorisant ainsi la stabilisa-
tion de la liaison au ligand et l’activation de la trans-
mission du signal intracellulaire sous-jacent tel que
celui de la voie des mitogen-activated protein kinase
(MAPK) et des phosphatidylinositol-3 kinases (PI3K)
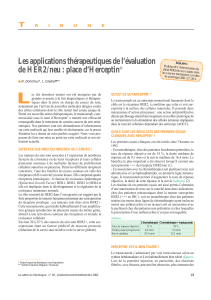
[figure 1] (2).
Son activation, en particulier dans les cancers du sein,
est essentiellement liée à une amplifi cation qui a pour
conséquence d’entraîner une surexpression de la pro-
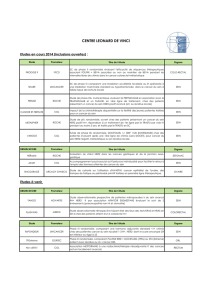
téine à la surface des cellules (fi gure 2). Cette amplifi ca-
tion concerne le gène HER2 et les gènes qui l’entourent
sur le bras long du chromosome 17 tels que STARD3,
GRB7, PNMT, PERLD1 (3, 4).
Les anomalies de nombres des chromosomes sont
les altérations génomiques les plus fréquentes dans
les carcinomes mammaires. Il est donc vite apparu
important de distinguer les anomalies de nombre du
chromosome 17 pouvant survenir dans le processus
de carcinogenèse des réelles amplifi cations visant à
activer l’oncogène HER2, elles seules étant indicatrices
de thérapie anti-HER2 aujourd’hui.
Détermination du statut de HER2
dans les carcinomes mammaires
Les méthodes de détermination du statut de HER2
doivent suivre les recommandations internationales et
nationales qui donnent des règles précises à appliquer
le plus scrupuleusement possible (5, 6).
La technique de première ligne est l’immunohisto-
chimie (IHC). Préalablement à son utilisation en pra-
tique clinique, il est recommandé que cette technique
soit calibrée sur l’amplifi cation du gène avec une
concordance de plus de 95 % entre les 2 approches.
Le laboratoire doit pouvoir prouver les résultats de
sa calibration et son adhésion à des organismes de
contrôle de qualité tels que l’Association française
d’assurance qualité en anatomie et cytologie patho-
logiques (AFAQAP) ou le United Kingdom National
External Quality Assessment Service (UK NEQUAS).
Les résultats de l’IHC identifi ent 3 scores de HER2 :
scores 0 et 1+ avec 10 % de cellules ayant un mar-
quage d’intensité faible et incomplet ; score 3+ avec
plus de 30 % de cellules marquées comportant un
marquage d’intensité forte et complet ; score 2+ avec
au moins 10 % de cellules marquées (≥ 10 %) avec
Figure 1. Voies de signalisation en aval des récepteurs de la famille EGFR et en particulier HER2
et HER3 (2).
PIP3PIP2
PI3K
p110
Ligands
ERBB3
ERBB2
Membrane
cytoplasmique
externe
Régions de dimérisation
P
P
P
PP
PP
P
PPPTEN
RAS
RAF
MEK
MAPK
Sos GRB2 Shc
mTOR
PDK1
NF-κB GSK3βp27
p85
AKT
BAD
Membrane nucléaire
Cycline D1 et cycline D2
MYC
VEGFA
Angiogenèse Prolifération Contrôle du
cycle cellulaire Suppression
de l’apoptose Survie
P
P
II
II II
III III
IV IV
C
NC
N

Correspondances en Onco-Théranostic - Vol. I - n° 2 - avril-mai-juin 2012
59
HER2 et cancers du sein
un marquage d’intensité faible ou modérée mais
complet (tableau I). Ces résultats d’IHC doivent être
interprétés dans une manipulation faite suivant un
protocole validé, avec un témoin multitissulaire aux
nombres de copies du gène HER2 connus (témoin à
2 copies, témoin amplifi é à faible niveau et témoin
amplifi é à fort niveau).
Les scores 2+ sont aussi appelés “cas équivoques” et
comprennent également les cas avec une surexpression
hétérogène de HER2. Les carcinomes avec un score 2+
doivent avoir une détermination du statut du gène
HER2 par hybridation in situ afi n que les cas amplifi és
pouvant bénéfi cier d’un traitement anti-HER2 soient
déterminés.
La détermination du statut du gène HER2 se fait par
hybridation in situ en fl uorescence ou en révélation ana-
lysable en lumière optique (grains d’argent pour la sonde
HER2 et chromogène rouge pour le centromère du chro-
mosome 17 ; INFORM HER2 Dual ISH assay, Ventana®).
Les seuils de positivité pour l’amplifi cation sont égale-
ment défi nis par le Collège des pathologistes américains
(6). Une tumeur est considérée comme amplifi ée pour
HER2 si, sur au moins 20 noyaux de cellules carcinoma-
teuses infi ltrantes, le ratio HER2/centromère du chro-
mosome 17 est supérieur à 2 ou le nombre de signaux
de HER2 seul supérieur à 6.
La fiabilité de la détermination du statut de HER2
proposée par des tests commerciaux fondés sur des
techniques de PCR quantitative à partir d’ADN extraits
de coupes tissulaires tumorales (Oncotype DX®, par
exemple) a récemment été remise en cause (7).
Taux de surexpression de HER2
des carcinomes infi ltrants
Les taux de surexpression de HER2 sont diff érents en
fonction du stade, de la taille, du grade, du statut gan-
glionnaire axillaire (N) et du type histologique du car-
cinome infi ltrant (tableau II). Le taux de surexpression
moyen (scores 3+ et 2+ amplifi és) des tumeurs T1a -T2
de moins de 3 cm est de 9 à 13 % (8-10).
Cette surexpression est dans la majorité des cas homo-
gène à toutes les cellules tumorales. Néanmoins, des cas
classés dans les cas équivoques “hétérogènes” montrent
la coexistence de 2 contingents intratumoraux, l’un
surexprimant HER2 avec une intensité forte et un mar-
quage complet et l’autre complètement négatif. Ces
cas sont très rares (11) et nécessitent de tester, le cas
échéant, les éventuelles métastases ganglionnaires
axillaires ou viscérales avant toute décision de traite-
ment anti-HER2 (6).
Tableau I. Interprétation et scores de la surexpression par immunohistochimie de la protéine HER2.
Score Marquage Indication pour le trastuzumab
0 Absence de marquage ou < 10 %
de cellules
Non
+ Marquage faible et incomplet
de>10 % de cellules
Non
++ Marquage faible ou modéré et complet
de ≥ 10 % de cellules
Oui, seulement si amplifi cation
prouvée par FISH/CISH/SISH
+++ Marquage fort et complet de > 30 %
de cellules
Oui
Tableau II. Taux d’HER2 (3+) diff érents en fonction des types histologiques et du stade (5, 8-10).
Canalaires Autres types
T1a, b : < 1 cm 9 % Lobulaire < 5 %
< 2 cm 10-15 % Tubulaire 0 %
> 2 cm 20-25 % Médullaire, basal-like 0 %
Grade I 5 % BRCA1 0 %
Grade II 10-17 % BRCA2 6 %
Grade III 29 % Cancer infl ammatoire 30 %
N- 9-20 % Cancer du sein (homme) 11 % à 30 %
N+ 1-3 16-21 %
N+ ≥ 4 28 %
Figure 2. A : amplifi cation du gène HER2 détectée par
FISH (signaux rouges : HER2 ; signaux verts : centromères
du chromosome 17). B : détection par immunohistochimie
de la surexpression membranaire forte de plus de 30 %
de cellules carcinomateuses avec un marquage complet
circonférentiel.
A
B

Correspondances en Onco-Théranostic - Vol. I - n° 2 - avril-mai-juin 2012
60
dossier thématique
Marqueurs prédictifs
de sensibilité et
de résistance aux anti-HER
Stabilité du taux de HER2 entre la tumeur
primaire et les métastases
Entre 1988 et 2012, plus de 30 études ont analysé la
stabilité des récepteurs hormonaux et de HER2 entre les
sites primaires et secondaires. Les variations de statut
pour HER2 sont rapportées dans 7,7 % des cas (métas-
tases ganglionnaires et viscérales) et 7,1 % des cas si
seules les métastases viscérales sont considérées (12-14).
En pratique, la détermination du statut de HER2 est
réalisée sur la tumeur primaire pour la défi nition du
traitement en adjuvant (après la chirurgie). Si l’indication
de traitement anti-HER2 est posée devant une situation
clinique métastatique, il est souhaitable d’eff ectuer une
biopsie de la lésion métastatique si elle est accessible
cliniquement, afi n de confi rmer le statut HER2 des cel-
lules métastatiques ainsi que le statut des récepteurs
hormonaux.
Un ou plusieurs types de carcinomes HER2
amplifi és ?
Les carcinomes HER2 amplifi és ont, depuis 10 ans, fait
l’objet de nombreuses analyses génomiques, phéno-
typiques et transcriptomiques. Il est maintenant clair que
plusieurs types de carcinomes HER2 amplifi és existent,
défi nis par le statut des récepteurs aux estrogènes, le
type d’altérations génomiques associées ou la nature
du stroma.
L’amplification d’HER2 est liée, dans environ 50 %
des cas, à l’absence d’expression des récepteurs aux
estrogènes. Les carcinomes HER2 avec récepteurs aux
estrogènes négatifs présentent une expression forte
de nombreux gènes de prolifération, sont pour la plu-
part de grade 3 et ont un taux de mutations du gène
TP53 de l’ordre de 75 % (15, 16). Dans les analyses non
supervisées des données transcriptomiques, les car-
cinomes HER2 amplifi és avec ou sans expression des
récepteurs aux estrogènes forment 2 clusters distincts,
mais ceux avec récepteurs aux estrogènes positifs sont
mêlés aux carcinomes de type luminal B (15, 16). Il faut
noter également que les tumeurs HER2 amplifi ées avec
récepteurs aux estrogènes positifs ne présentent une
positivité des récepteurs à la progestérone que dans
25 % des cas (8, 17).
Les profi ls génomiques des carcinomes HER2 amplifi és
sont en particulier caractérisés par d’autres régions
d’amplifi cations situées entre autres à la partie plus
télomérique du bras long du chromosome 17 ou sur
d’autres chromosomes (8q, 11q…) [4, 18]. Récemment,
il a été montré que les carcinomes HER2 amplifi és, asso-
ciés ou non à l’expression des récepteurs aux estro-
gènes, appartiennent à l’entité moléculaire apocrine
(19), caractérisés entre autres par de nombreuses alté-
rations de nombres des chromosomes et l’expression
des récepteurs aux androgènes.
Les carcinomes HER2 amplifi és forment également
2 groupes de pronostic diff érent en fonction de la
richesse en lymphocytes de leur stroma. Les tumeurs
HER2 amplifi ées et associées à une signature trans-
criptomique immune et dont le stroma présente un
fort infi ltrat lymphocytaire ont un meilleur pronostic
(20).
Paramètres de réponse
aux thérapies anti-HER2
Les thérapies ciblées anti-HER2 sont dans la majorité
des cas associées à des chimiothérapies cytotoxiques
classiques. Ainsi, les paramètres prédictifs de réponse
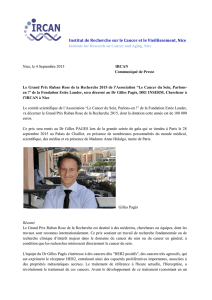
Figure 3. A : fort niveau d’amplifi cation de HER2 ; amas
de signaux rouges, signant l’amplifi cation de HER2 en pré-
sence d’un polysomie du centromère du chromosome 17
(signaux verts). B : faible niveau d’amplifi cation de HER2 ;
6 à 8 copies de HER2 (signaux rouges et centromères du
chromosome 17 en vert (1 à 2 signaux).
A
B

Correspondances en Onco-Théranostic - Vol. I - n° 2 - avril-mai-juin 2012
61
HER2 et cancers du sein
classiques comme le grade, la prolifération et la néga-
tivité des récepteurs hormonaux sont à prendre en
considération dans l’évaluation de la possibilité de
réponse d’une tumeur HER2 amplifi ée à la chimio-
thérapie. Ensuite, le critère majeur de réponse aux
thérapies anti-HER2 est le niveau d’amplifi cation de
HER2. En situation néo-adjuvante, il a été montré
qu’une réponse histologique complète était obtenue
dans 22 % des tumeurs présentant un faible niveau
d’amplifi cation du gène HER2 (compris entre 6 et
10 copies) contre un taux de réponse complète de
56 % lorsque l’amplifi cation était de plus de 10 copies
(21) [figure 3].
Les autres mécanismes connus de non-réponse aux
anti-HER2 sont les mécanismes d’activation des voies
de transduction du signal indépendantes de HER2
telles que les mutations de PI3KCA observées dans 22
à 33 % des carcinomes HER2 amplifi és, en particulier
ceux avec récepteurs aux estrogènes positifs, ou les
pertes de PTEN surtout observées dans les carcinomes
avec récepteurs aux estrogènes négatifs (22-24). Les
analyses pangénomiques fi nes par séquençage massif
permettront encore mieux d’affi ner les critères de
réponses (25).
Conclusion
Les taux d’amplifi cation de HER2 dans les cancers du
sein varient de 9 à 30 % en fonction du stade, du grade,
du type histologique et de N. La détermination du statut
de HER2 dans les cancers du sein en pratique clinique
répond à de nombreuses règles soumises à un contrôle
de qualité externe indispensable pour assurer la fi abilité
et la reproductibilité des tests utilisés.
Plusieurs types de carcinomes HER2 ont été reconnus
comme étant diff érents sur le plan génomique, phéno-
typique ou stromal. Ces diff érences modulent l’impact
pronostique de l’amplifi cation de HER2 et doivent être
prises en considération pour dessiner les futurs essais
cliniques visant à améliorer les performances théra-
peutiques des thérapies ciblées anti-HER2.
■
1. Slamon D, Clarck G, Wong S. Human breast cancer:
Correlation of relapse and survival with amplifi cation of the
HER-2/neu oncogene. Science 1987;235:177-81.
2.
Baselga J, Swain SM. Novel anticancer targets: revisiting
ERBB2 and discovering ERBB3. Nat Rev Cancer 2009;9(7):463-75.
3. Kauraniemi P, Kuukasjarvi T, Sauter G, Kallioniemi A.
Amplifi cation of a 280-kilobase core region at the ERBB2 locus
leads to activation of two hypothetical proteins in breast can-
cer. Am J Pathol 2003;163(5):1979-84.
4.
Staaf J, Jonsson G, Ringner M et al. High-resolution genomic
and expression analyses of copy number alterations in HER2-
amplifi ed breast cancer. Breast Cancer Res 2010;12(3):R25.
5. Penault-Llorca F, Vincent-Salomon A, Bellocq JP et al. Mise
à jour des recommandations du GEFPICS pour l’évaluation du
statut HER2 dans les cancers du sein en France. Ann Pathol
2010;30(5):357-73.
6. Wolff AC, Hammond ME, Schwartz JN et al. American Society
of Clinical Oncology/College of American Pathologists guideline
recommendations for human epidermal growth factor receptor
2 testing in breast cancer. J Clin Oncol 2007;25(1):118-45.
7. Dabbs DJ, Klein ME, Mohsin SK, Tubbs RR, Shuai Y, Bhargava
R. High false-negative rate of HER2 quantitative reverse
transcription polymerase chain reaction of the Oncotype DX
test: an independent quality assurance study. J Clin Oncol
2011;29(32):4279-85.
8. Bartlett JM, Ellis IO, Dowsett M et al. Human epidermal
growth factor receptor 2 status correlates with lymph node
involvement in patients with estrogen receptor (ER) negative,
but with grade in those with ER-positive early-stage breast
cancer suitable for cytotoxic chemotherapy. J Clin Oncol
2007;25(28):4423-30.
9. Rodrigues MJ, Wassermann J, Albiges L et al. Trastuzumab
treatment in t1ab, node-negative, human epidermal growth
factor receptor 2-overexpressing breast carcinomas. J Clin
Oncol 2010;28(28):e541-2.
10. Ignatiadis M, Sotiriou C. Breast cancer: Should we assess
HER2 status by Oncotype DX? Nat Rev Clin Oncol 2012;9(1):12-4.
11. Cottu PH, Asselah J, Lae M et al. Intratumoral heterogeneity
of HER2/neu expression and its consequences for the mana-
gement of advanced breast cancer. Ann Oncol 2008;19(3):
595-7.
12. Wu JM, Fackler MJ, Halushka MK et al. Heterogeneity of
breast cancer metastases: comparison of therapeutic tar-
get expression and promoter methylation between primary
tumors and their multifocal metastases. Clin Cancer Res
2008;14(7):1938-46.
13. Vincent-Salomon A, Bidard FC, Pierga JY. Bone mar-
row micrometastasis in breast cancer: review of detection
methods, prognostic impact and biological issues. J Clin Pathol
2008;61(5):570-6.
14.
Vincent-Salomon A, Jouve M et al. HER2 status in patients
with breast carcinomas is not modifi ed selectively by preo-
perative chemotherapy and is stable during the metastatic
process. Cancer 2002;94:2169-73.
15. Sorlie T, Perou CM, Tibshirani R et al. Gene expression pat-
terns of breast carcinomas distinguish tumor subclasses with
clinical implications. PNAS 2001;98(19):10869-74.
16. Sorlie T, Tibshirani R, Parker J et al. Repeated observation
of breast tumor subtypes in independent gene expression data
sets. PNAS 2003;100(14):8418-23.
17. Konecny G, Pauletti G, Pegram M et al. Quantitative asso-
ciation between HER-2/neu and steroid hormone receptors in
hormone receptor-positive primary breast cancer. JNCI Cancer
Spectrum 2003;95(2):142-53.
18. Jonsson G, Staaf J, Vallon-Christersson J et al. Genomic
subtypes of breast cancer identifi ed by array-comparative
genomic hybridization display distinct molecular and clinical
characteristics. Breast Cancer Res 2010;12(3):R42.
19. Guedj M, Marisa L, de Reynies A et al. A refi ned molecular
taxonomy of breast cancer. Oncogene 2011;31(9):1196-206.
20.
Staaf J, Ringner M, Vallon-Christersson J et al. Identifi cation
of subtypes in human epidermal growth factor receptor 2--posi-
tive breast cancer reveals a gene signature prognostic of out-
come. J Clin Oncol 2010;28(11):1813-20.
21.
Arnould L, Arveux P, Couturier J et al. Pathologic com-
plete response to trastuzumab-based neoadjuvant therapy
is related to the level of HER-2 amplifi cation. Clin Cancer Res
2007;13(21):6404-9.
22.
Saal LH, Gruvberger-Saal SK, Persson C et al. Recurrent
gross mutations of the PTEN tumor suppressor gene in breast
cancers with defi cient DSB repair. Nat Genet 2008;40(1):102-7.
23.
Saal LH, Holm K, Maurer M et al. PIK3CA Mutations cor-
relate with hormone receptors, node metastasis, and ERBB2,
and are mutually exclusive with PTEN loss in human breast
carcinoma. Cancer Res 2005;65(7):2554-9.
24. Dave B, Migliaccio I, Gutierrez MC et al. Loss of phosphatase
and tensin homolog or phosphoinositol-3 kinase activation
and response to trastuzumab or lapatinib in human epidermal
growth factor receptor 2-overexpressing locally advanced
breast cancers. J Clin Oncol 2010;29(2):166-73.
25. Barretina J, Caponigro G, Stransky N et al. The cancer cell
line encyclopedia enables predictive modelling of anticancer
drug sensitivity. Nature 2012;483(7391):603-7.
Références
Liens d’intérêts.
L’auteur déclare
avoir perçu des honoraires de
Roche pour des cours et des par-
ticipations à des boards.
1
/
5
100%