Club Médecine interne et oeil

123456478389254954A5BC56
DE4F59
26834B8354233545
Club Médecine Interne et Œil
FMC du 4 octobre 201

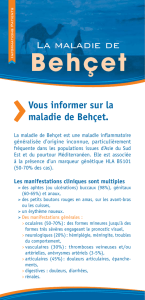
Maladie de Behçet

12345678962ABCDEFA9
29A96553A9B7E7698A9

1234564A5BC564
38625444449548
423868328624448
264

Critères diagnostiques
• Ulcérations orales récurrentes: récidivant plus de 3 fois
en 12 mois
• + 2 des manifestations suivantes:
– ulcérations génitales récurrentes
– lésions cutanées
– test pathergique positif
– Uvéite
• Critères applicables uniquement en l’absence d’autres
explications cliniques
INTERNATIONAL STUDY GROUP FOR BEHÇET’S DISEASE. Criteria for diagnosis of Behçet’s disease. Lancet, 1990, 335: 1078-1080
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
1
/
48
100%