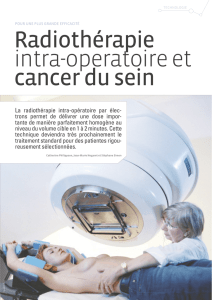
Radiothérapie

LA RADIOTHÉRAPIE CHEZ LE
SUJET ÂGÉ
Dr Baret Aurélie

Epidémiologie
Augmentation de l’espérance de vie
Plus de la moitié des patients
atteints de cancer ont plus de 65 ans

Problématique
Le pronostic des cancers du sujet âgé est plus
péjoratif (par rapport au sujet jeune) du fait :
D’un diagnostic plus tardif
De ses co-morbidités
Et d’une prise en charge sub-optimale


Problématique
Patients âgés
SOUS TRAITES
à cause de notre
PATERNALISME
Patients âgés
SUR TRAITES
à cause des
GUIDELINES
Sélectionner les patients FIT aptes pour un traitement classique
Sélectionner les patients UNFIT pour leur proposer un traitement adapté
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
1
/
28
100%