David Vancraeynest Congrès UCL de médecine générale Mai 2014

David Vancraeynest
Cardiologie
Congrès UCL de médecine générale
Mai 2014

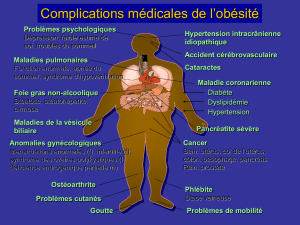
Introduction
Le traitement pharmacologique
La prise en charge des facteurs de risque
Tabac
Diabète et le contrôle glycémique
Hypertension artérielle et le contrôle tensionnel
Cholestérol
La pratique du sport / La réadaptation pour cardiaque
Facteurs psychosociaux

Introduction
Le traitement pharmacologique
La prise en charge des facteurs de risque
Tabac
Diabète et le contrôle glycémique
Hypertension artérielle et le contrôle tensionnel
Cholestérol
La pratique du sport / La réadaptation pour cardiaque
Facteurs psychosociaux

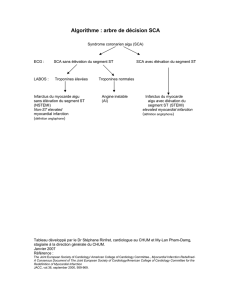
It is THROMBOSIS, superimposed on ruptured
plaque that precipitates life-threatening clinical
events
ACS
Stroke

Approximately one third of STEMI
patients die within 24 hours of onset
of ischemia.
The morbidity and mortality is lower
in UA/NSTEMI patients, but is still
substantial, and about 15% of
patients die or experience a
reinfarction within 30 days of
diagnosis.
Circulation. 2004;110(9):e82-e292
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
1
/
35
100%