La présence de CTC et/ou d`ADN circulant change-t

Personnaliser les traitements
médicaux en situation non
métastatique:
La présence de CTC et/ou d’ADN
circulant change-t-elle la décision?
Jean-Yves Pierga
Département d’Oncologie médicale
Institut Curie

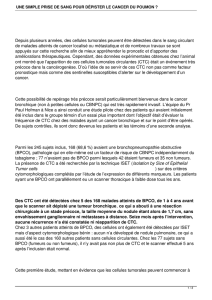
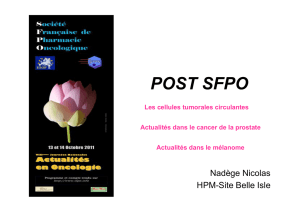
Etapes de la dissémination métastatique et de la survie
des cellules tumorales circulantes CTC
Kang Y Cancer Cell 23, 2013


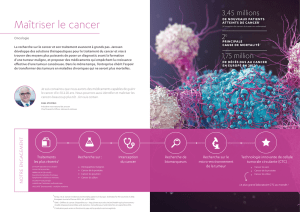
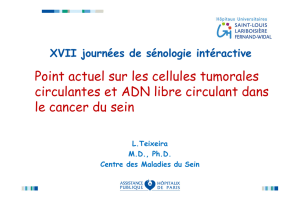
Multiples techniques de détection des CTC
Alix-Panabières C. NATURE REVIEWS CANCER 14, 2014, 623

Selection positive EPCAM
Staining : CK 8/18/19, CD45, DAPI
others: HER2/Neu, MUC1, EGF-R)
Epithelial
Cell
Epithelial
Cell
CK
Y
Anti-
CK-PE
CK
Y
CK
Y
Anti-
CK-PE
Nucleus
DAPI
Nucleus
DAPI
Nucleus
DAPI
Y
EpCAM
Anti-EpCAM
Ferrofluid
Y
EpCAM
Y
EpCAM
Anti-EpCAM
Ferrofluid
LeukocyteLeukocyte
Y
CD45
Anti -
CD45-APC
Y
CD45
YY
CD45
Anti -
CD45-APC
Nucleus
DAPI
Y
EpCAM
Nucleus
DAPI
Y
EpCAM
Nucleus
DAPI
Nucleus
DAPI
Nucleus
DAPI
Y
EpCAM
Y
EpCAM
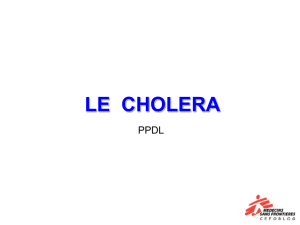
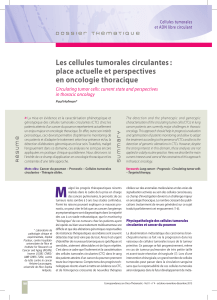
CellSearch™ System FDA cleared
Détection des cellules tumorales circulantes
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
1
/
39
100%