CANCERS DU SEIN HER2+ LA BELLE HISTOIRE CAEN 2014

CANCERS DU SEIN HER2+
LA BELLE HISTOIRE
CAEN 2014
Pr Jean-Philippe SPANO
Hôpital Pitié-Salpêtrière, Paris

•Disclosure form:
•Consultant or advisory role (fees) or
meeting invitation from Cephalon, TEVA
Pharma, Roche, MSD, Merck-Serono,
Sanofi, Amgen, GSK, Vifor, PFO, Leo
Pharma and Gilead

Shc
PI3K
Raf
MEKK-1
MEK
MKK-7
JNK ERK
Ras
mTOR
Grb2
AKT
Sos-1
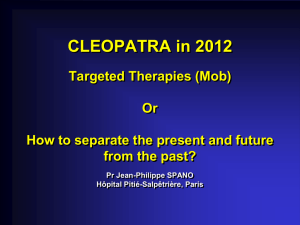
EGFR activation
mediates multiple
processes
EGF Pathway
Adapted from:
Ciardiello F, et al. N Engl J Med. 2008;358:1160-1174.


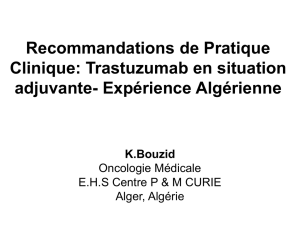
HER2 dans les cancers du sein
Type de tumeurs Surexpression
ErbB1 (%)
Surexpression
ErbB2 (%)
Vessie 31%-48% 7%-36%
Sein 14%-91% 10%-37%
Colorectal 25%-77% 7%
Oesophage 71% 13%-73%
Gliomes 40%-50% –
CBNPC 40%-80% 3%-56%
Ovaire 30%-75% 20%-32%
Pancréas 30%-50% –
Rein 50%-90% 24%-40%
ORL 30%-75% 32%-62%
Estomac – 5%-55%
La surexpression de HER2 varie de 10% à 37%, avec une médiane aux environs de 20%
Fumoleau P et al. Bull Cancer 2007; 94(7):F147-70
Données à partir de biopsies tumorales
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
1
/
69
100%