Prise en charge nutritionnelle des cancers digestifs au cours

16 | La Lettre de l’Hépato-gastroentérologue • Vol. XVI - n° 1 - janvier-février 2013
DOSSIER THÉMATIQUE
Cancer et nutrition
Prise en charge nutritionnelle
des cancers digestifs au cours
de la chimiothérapie (à visée
curative ou palliative) et en
situation palliative avancée
Nutritional care for digestive cancers in curative and
palliative chemotherapy and in advanced palliative situation
Pascal Crenn*
*Unité de nutrition clinique, départe-
ment de médecine aiguë spécialisée,
EA 4497 (UVSQ), hôpital Raymond-
Poincaré (APHP), Garches.
L
a chimiothérapie et la maladie tumorale sous-
jacente entraînent des complications nutrition-
nelles et des difficultés alimentaires. Celles-ci
sont responsables de carences, et la dénutrition
augmente la toxicité, en particulier hématologique,
de la chimiothérapie (1). Néanmoins, il n’existe pas
à l’heure actuelle d’études démontrant clairement
le bénéfice de la prise en charge nutritionnelle pour
diminuer les complications des chimiothérapies, et
des biothérapies, ou pour améliorer la survie des
patients en cours de traitement. Selon l’ASPEN (2),
le support nutritionnel artificiel, à la différence
des conseils diététiques, ne doit pas être utilisé
systématiquement chez les patients en cours de
chimiothérapie. Ce support est conseillé si le patient
est dénutri et/ou dans l’incapacité de s’alimenter
pendant une durée de 7 à 14 jours (grade B, ASPEN).
En cas de mucite sévère en rapport avec le traite-
ment, la nutrition parentérale de courte durée paraît
logique mais elle n’a jamais fait l’objet d’une étude
qui la compare à une nutrition entérale (3). Les
principales recommandations, tirées de l’analyse
de la littérature, sont indiquées dans le paragraphe
spécifique et sur les gures1et2. Deux situations
peuvent être individualisées :
➤
chimiothérapie d’une néoplasie digestive effec-
tuée à visée curative ;
➤
situations palliatives, comportant ou non (situa-
tions palliatives avancées) une chimiothérapie.
Les néoplasies autres que digestives ne seront ici
que très ponctuellement évoquées.
Chimiothérapie à visée curative
Conseils diététiques personnalisés
et compléments nutritionnels oraux
Une étude multicentrique randomisée a évalué
l’impact d’une intervention nutritionnelle sur la
tolérance de 3 mois de chimiothérapie associant
5-FU et méthotrexate dans les cancers colorectaux
non résécables (n = 90) et les cancers du poumon
(n = 102) [4]. Les patients étaient randomisés en
3 groupes : un groupe contrôle (apports alimentaires
libres), un groupe “intervention diététique stan-
dard” (avec conseils permettant la couverture de
1,7 à 1,95 fois la dépense énergétique de base selon
le statut nutritionnel), et un groupe “intervention
nutritionnelle renforcée” recevant des conseils simi-
laires au groupe précédent avec une alimentation
enrichie à 25 % de protéines et supplémentée en
zinc (150 mg/j) et en magnésium (266 mg/j). Les
interventions nutritionnelles personnalisées ont
permis l’augmentation des apports énergétiques et
protéiques durant tout le cycle de chimiothérapie par
rapport aux données de base, comparées au groupe
contrôle (p < 0,001 pour le cancer du poumon ;

La Lettre de l’Hépato-gastroentérologue • Vol. XVI - n° 1 - janvier-février 2013 | 17
Points forts
»En cours de chimiothérapie et en présence d’une dysgueusie et/ou d’une anorexie, il est recommandé
un conseil diététique personnalisé intégrant, en cas de dénutrition et/ou de diminution des ingesta, des
compléments nutritionnels oraux.
»
La nutrition artificielle n’est pas recommandée si l’état nutritionnel et/ou les ingesta restent satisfaisants.
Il n’y a pas de preuves qu’elle diminue la fréquence des toxicités des traitements. Son utilisation doit être
discutée au cas par cas et avec le patient, et la voie entérale sera privilégiée. La nutrition parentérale n’est
à proposer que si le tube digestif est inutilisable ou inaccessible.
»
Dans les situations palliatives et palliatives avancées, l’objectif est la qualité de vie et le traitement
des symptômes associés à la dénutrition. Quand le facteur limitant n’est plus l’évolution tumorale mais
l’absence d’apport nutritif, un support nutritionnel est recommandé.
Mots-clés
Chimiothérapie
Dénutrition
Compléments
nutritionnels oraux
Nutrition entérale
Nutrition parentérale
Highlights
»
During chemotherapy and
in the presence of dysgeusia
and/oranorexia,anintegrating
personalized dietary advice is
recommended with oral nutri-
tional supplements in cases of
malnutritionand/ordecreased
food intake.
»
Artificial nutrition is not
recommended if the nutri-
tionalstatusand/ororalintake
remain satisfactory. There is no
evidence that artificial nutrition
reduces the toxicities of treat-
ment. Its use has to be
»
Discussed case by case with
the patient, and enteral has to
be privileged. Parenteral nutri-
tion is to propose only if the
digestive tract is unusable or
inaccessible.
»
In palliative situations and
advanced palliative cases, the
goal is quality of life and the
treatment of symptoms associ-
ated with undernutrition. When
the limiting factor is no longer
tumor progression but
the absence of nutrients
intake, nutritional support is
recommended.
Keywords
Chemotherapy
Undernutrition
Oral nutritional supplements
Enteral nutrition
Parenteral nutrition
p < 0,004 pour le cancer colorectal) [4]. Le conseil
diététique personnalisé n’entraînait pas de varia-
tion significative du poids par rapport au groupe
contrôle (4). Aucune différence significative n’a été
démontrée sur la réponse tumorale, les doses de
chimiothérapies administrées, les degrés de toxicité,
la fréquence de retard des traitements, la survie et
la qualité de vie (4).
De manière générale, il importe de prendre en
compte les symptômes (anomalies du goût, troubles
de la déglutition, troubles digestifs, etc.) de façon à
améliorer l’appétit. De nombreux articles ont décrit
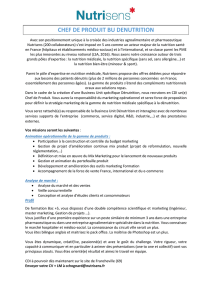
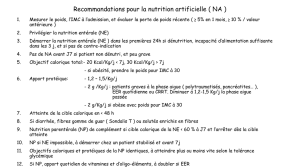
Dans toutes les situations :
Pesée systématique
Pourcentage de perte de poids*
IMC**
Évaluation des ingesta
Utilisation d’index possible :
SGA
MNA
(pour les personnes âgées)
Patient non
dénutri
Patient dénutri***
et/ou ingesta
bas
Pas de conseil diététique systématique
La nutrition artificielle n’est pas recommandée
Conseil diététique ± compléments nutritionnels
oraux
Nutrition artificielle au cas par cas en favorisant
la nutrition entérale
La nutrition parentérale n’est recommandée que
si le tube digestif (intestin grêle) est inutilisable
ou inaccessible
* Perte de poids : notifier en pourcentage le delta entre le poids actuel et le poids habituel ou le poids de forme ou celui relevé dans les 6 mois qui
ont précédé le diagnostic. Une perte de poids ≥ 5 % définit la dénutrition dans cette situation.
** Indice de masse corporelle : il ne doit pas être utilisé seul par manque de sensibilité ; l'IMC est significatif si < 18,5 ou < 21 pour les
personnes âgées de 70 ans ou plus.
*** Perte de poids ≥ 5 % ; IMC < 18,5 ou < 21 pour les personnes âgées de 70 ans ou plus.
Figure 1. Nutrition en situation de chimiothérapie à visée curative.
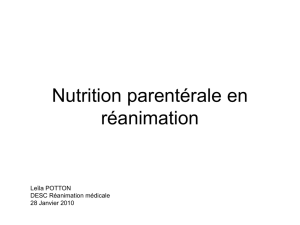
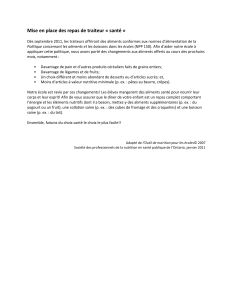
Patient non
dénutri
Patient dénutri***
et/ou ingesta
bas
Pas de conseil diététique systématique
La nutrition artificielle n’est pas
recommandée
Conseil diététique ± compléments
nutritionnels oraux
Nutrition artificielle au cas par cas
en favorisant la nutrition entérale
La nutrition artificielle doit être discutée
et tracée
La nutrition parentérale est recommandée
si le tube digestif (intestin grêle) est
inutilisable ou inaccessible (cas typique :
carcinose péritonéale)
* Perte de poids : notifier en pourcentage le delta entre le poids actuel et le poids habituel ou le poids de forme celui relevé dans les 6 mois qui
ont précédé le diagnostic. Une perte de poids ≥ 5 % définit la dénutrition dans cette situation.
** Indice de masse corporelle : il ne doit pas être utilisé seul par manque de sensibilité ; l'IMC est significatif si < 18,5 ou < 21 pour les
personnes âgées de 70 ans ou plus.
*** Perte de poids ≥ 5 % ; IMC < 18,5 ou < 21 pour les personnes âgées de 70 ans ou plus.
Dans toutes les situations :
Pesée systématique
Pourcentage de perte de poids*
IMC**
Évaluation des ingesta***
Utilisation d’index possible :
SGA
MNA (pour les personnes âgées)
Figure 2. Nutrition en situation palliative et palliative avancée.

18 | La Lettre de l’Hépato-gastroentérologue • Vol. XVI - n° 1 - janvier-février 2013
DOSSIER THÉMATIQUE
Cancer et nutrition Prise en charge nutritionnelle en chimiothérapie
et en situation palliative avancée
les effets indésirables des traitements antinéopla-
siques mais aussi des traitements associés tels que les
analgésiques opiacés ou les antibiotiques. Certaines
carences en oligoéléments peuvent avoir un effet
délétère sur l’appétit et le transit digestif. En cours
de chimiothérapie, l’asthénie, les nausées, les vomis-
sements, les mucites, les sécheresses buccales, les
diarrhées, la constipation mais aussi les altérations
du goût (dysgueusie et agueusie), de l’odorat (hype-
rosmie, hyposmie), la plainte concernant un arrière-
goût métallique, une hypersensibilité au sucré, au
salé, à l’acide et à l’amer peuvent être responsables
d’aversions alimentaires. Néanmoins, ces symptômes
sont subjectifs, complexes et très variables selon les
patients (5). Ces derniers décrivent les difficultés et
les sensations qui entraînent une baisse de l’appétit,
un dégoût alimentaire et une satiété précoce. Pour
mettre en évidence l’effet des modifications de
goût sur la consommation alimentaire, une étude a
comparé 30 patients après le second cycle de chimio-
thérapie à 30 témoins
(6). Les modifications de goût
ont été relevées ainsi que les quantités d’aliments
consommées. Deux saveurs (sucré, amer) de concen-
trations différentes ont servi de tests. Les patients
en cours de traitement avaient une perception du
sucré et de l’amer supérieure à celle du groupe témoin
(seuils de perception de respectivement 6,4 versus
4,4 μmol/ml [p = 0,03], et de 100 versus 95 μmol/
ml [p = 0,04]), et les consommations énergétiques et
protéiques étaient diminuées (respectivement 2 043
versus 1 586 kcal [p = 0,02] et 81,4 versus 54 g/j
[p = 0,01]) chez les patients.
En ce qui concerne les compléments nutritionnels
oraux (CNO), une étude a évalué 111 patients traités
par radiothérapie et chimiothérapie préopératoires
pour cancer colorectal (7). La prise quotidienne
de 2 CNO hyperprotéinés permettait, de façon
significative, l’augmentation des apports protéino-
énergétiques, l’amélioration de l’état nutritionnel
et de la qualité de vie des patients et la réduction
de la toxicité du traitement. Cependant, l’efficacité
des CNO était inférieure à celle observée avec les
seuls conseils diététiques “proactifs” et renforcés.
De plus, l’augmentation des apports protéino-
énergétiques avec les CNO n’était constatée que
pendant la phase de prise en charge et disparaissait
après 3 mois.
Nutrition artificielle
Dans les études publiées sur la nutrition artificielle, le
plus souvent parentérale, les situations étudiées sont
habituellement celles de cancers au stade avancé,
donc de fait, dans la majorité des cas, elles sont non
curatives ; de plus, les groupes de patients y sont
hétérogènes, notamment quant à la présence ou
non d’une carcinose péritonéale. Pour ces raisons,
les bénéfices propres du support nutritionnel sont
difficiles à déterminer.
Les études de nutrition entérale chez les patients
porteurs d’un cancer et en cours de traitement
par chimiothérapie sont très peu nombreuses et
anciennes. Les recommandations publiées
(8)
indiquent que la nutrition entérale en cours de
chimiothérapie n’a pas d’effet sur la réponse tumo-
rale à la chimiothérapie, qu’elle ne diminue pas ses
effets indésirables et, de fait, qu’elle a une utilité
discutable (grade C, ESPEN). Il n’y a pas de compa-
raison publiée entre les sites gastriques et post-
duodénaux de nutrition entérale chez les patients
recevant une chimiothérapie émétisante. Une série
rétrospective non comparative indique cependant
que la voie post-pylorique permet, dans 92 % des
cas, la poursuite de la nutrition dans cette situa-
tion (9). Deux études concernant la nutrition enté-
rale au cours de la chimiothérapie sont disponibles.
Ces études ont analysé l’impact d’une nutrition
entérale versus une alimentation orale standard.
Elles ont porté sur des cancers digestifs avancés
(10, 11). La première étude date de 1984 (11). Elle
a concerné 70 patients, dont 62 étaient évaluables
(35 cancers hépato-biliaires, 16 carcinomes de
l’estomac et 11 carcinomes colorectaux)
[11]. Il
s’agissait d’une étude randomisée entre alimen-
tation orale et hypernutrition entérale au cours
de la chimiothérapie (1 800 calories les 2 premiers
jours suivies de 3 000 à 4 000 calories à partir du 3
e
jour). Il faut noter que ce deuxième groupe recevait
des apports probablement trop élevés. Pour les
patients en alimentation orale, après 3 semaines de
chimiothérapie, la perte de poids était significative
mais aucune variation significative des protéines
nutritionnelles n’était objectivée. Dans le groupe
nutrition entérale, il était noté une augmentation
significative du poids. La morbi-mortalité était
inférieure pour le groupe nutrition entérale par
rapport au groupe alimentation orale (11). Un autre
travail
(10), prospectif et non randomisé, a porté
sur 50 patients porteurs d’un cancer de l’œsophage
bénéficiant d’une chimiothérapie avec 5-FU et
cisplatine suivie d’une radiothérapie à visée cura-
tive. Vingt-neuf patients dysphagiques ont reçu une
nutrition entérale (37 kcal/kg/j, 0,32 g d’azote/kg/j
pendant 34 jours) et 21 patients non dysphagiques
ont reçu une alimentation orale standard. Les

La Lettre de l’Hépato-gastroentérologue • Vol. XVI - n° 1 - janvier-février 2013 | 19
DOSSIER THÉMATIQUE
patients ayant une nutrition entérale avaient perdu
significativement plus de poids que les patients
ayant une alimentation orale avant d’entrer dans
l’étude (16,8 % versus 12,8 % respectivement,
p < 0,02). L’apport de nutrition entérale a repré-
senté 86 % du support nutritionnel programmé.
Dans cette étude, la nutrition entérale a permis
une stabilité du poids, alors que, dans le groupe
alimentation orale, il a été noté une diminution
significative du poids ainsi que de l’albuminémie
(p < 0,01). Il n’y avait pas de différence entre les
2 groupes quant à la tolérance de la chimiothérapie
et à la réponse tumorale, avec une médiane de
survie de 9,5 mois.
Situations palliatives
et soins palliatifs avancés
Le support diététique reste bien entendu toujours
indiqué mais l’anorexie est fréquemment majeure. La
nutrition parentérale ou, plus rarement, entérale peut
être proposée chez le malade hypophagique et/ou
subocclus (12) [notamment par carcinose péritonéale]
Recommandations (issues du groupe de travail Nutrition et cancer
de la Société francophone Nutrition clinique et métabolisme)
Au cours de la chimiothérapie, les données actuelles ne permettent pas de recommander de façon systématique une consul-
tation ou un conseil diététique personnalisé (grade C). Cependant, en présence de troubles du goût et d’une anorexie, il est
recommandéunconseildiététiquepersonnaliséintégrantsinécessairelaprescriptiondeCNOencasdedénutritionet/oude
diminutiondesingesta,et/ouàlademandedupatientoudelafamille(avisd’experts).
Il n’y a pas de preuve incontestable établissant que la nutrition parentérale ou entérale diminue la survenue des toxicités des
traitements par chimiothérapie. En cas de nécessité de mise en place d’une nutrition artificielle, celle-ci devra intégrer le plan
personnalisé de soins en favorisant la nutrition entérale (avis d’experts). La nutrition artificielle systématique n’est ainsi pas
recommandée chez le patient en cours de chimiothérapie si l’état nutritionnel et/ou les ingesta restent satisfaisants
(grade A). En l’absence d’études probantes dans ce domaine, l’indication de la nutrition artificielle doit être discutée au cas par
cas et avec le patient, et la voie entérale devra être privilégiée (avis d’experts). Elle doit être idéalement discutée en réunion de
concertation pluridisciplinaire et inscrite dans le dossier.
La nutrition parentérale n’est recommandée que si le tube digestif (intestin grêle) est inutilisable ou inaccessible (grade C).
La complémentation systématique du mélange nutritif par des pharmaconutriments (par voie orale ou parentérale) n’est pas
recommandée (grade C).
Pouruneduréesupérieureà3semaines,etsiunegastrostomieestenvisagée,lachimiothérapiedevraitêtrepratiquéeàdistance
de la pose (un minimum de 15jours de délai avant et après la pose) en raison du risque infectieux (avis d’experts), la sonde
nasogastrique permettant d’alimenter le patient dans l’intervalle. En cas de nutrition parentérale, il est préférable d’utiliser des
perfusions discontinues et d’éviter les perfusions les jours de chimiothérapie intraveineuse (avis d’experts).
Dans les situations palliatives et palliatives avancées, l’objectif de la nutrition est la qualité de vie et le traitement des symptômes
associés à la dénutrition. Quand le facteur limitant n’est pas l’évolution tumorale mais l’absence d’apport nutritif, un support
nutritionnel est recommandé (avis d’experts). La mise en route d’une nutrition artificielle n’est pas recommandée si l’espérance
deviedupatientestinférieureà3moisetsil’atteintefonctionnellepermanenteestsévère(indicedeKarnofsky≤50%ou
PF≥3)[avisd’experts]. Dans ce contexte, la nutrition artificielle doit être discutée de façon multidisciplinaire. La décision doit
être inscrite dans le dossier du patient (avis d’experts). Une réévaluation après 15 jours est recommandée (avis d’experts).
avec dénutrition, dont l’espérance de vie prévisible
dépasse 3 mois ou en cas de demande spécifique du
patient ou de sa famille. Pour ce qui est des études pros-
pectives randomisées, nous ne disposons que d’un seul
travail en situation de chimiothérapie palliative. Dans
cette étude prospective randomisée de 152 patients
(13) ayant un cancer avancé (dans 85 % des cas d’ori-
gine digestive), 2 groupes ont été comparés. La moitié
recevait une nutrition parentérale de complément à
l’alimentation orale (avec CNO), et l’autre moitié cette
alimentation orale seule. Une amélioration significa-
tive de la qualité de vie, jugée sur le questionnaire de
l’EORTC QLQ-C30, mais aussi de la survie médiane
(9 versus 12,5 mois ; p < 0,05) et des paramètres nutri-
tionnels (indice de masse corporelle, albumine) a été
observée dans le groupe recevant une nutrition paren-
térale. Ce travail ne fournit cependant pas d’informa-
tions sur l’évolution ou non vers un syndrome occlusif
tout au long du suivi et du traitement nutritionnel, qui
a duré en moyenne 11 mois. La majorité des études
disponibles sont donc observationnelles. Huit études
d’effectifs et de localisations hétérogènes sont dispo-
nibles dans la littérature. Elles ne permettent pas de
conclusions pratiques fortes.

20 | La Lettre de l’Hépato-gastroentérologue • Vol. XVI - n° 1 - janvier-février 2013
DOSSIER THÉMATIQUE
Cancer et nutrition Prise en charge nutritionnelle en chimiothérapie
et en situation palliative avancée
1.Alexandre J, Gross-Goupil M, Falissard B et al. Evaluation
of the nutritional and inflammatory status in cancer patients
for the risk assessment of severe haematological toxicity
following chemotherapy. Ann Oncol 2003;14(1):36-41.
2.August DA, Huhmann MB. ASPEN clinical guidelines:
nutrition support therapy during adult anticancer treatment
and in hematopoietic cell transplantation. JPEN J Parenter
Enteral Nutr 2009;33(5):472-500.
3.Bozzetti F, Arends J, Lundholm K, Micklewright A, Zurcher
G, Muscaritoli M. ESPEN Guidelines on Parenteral Nutrition:
non-surgical oncology. Clin Nutr 2009;28(4):445-54.
4.Evans WK, Nixon DW, Daly JM et al. A randomized study of
oral nutritional support versus ad lib nutritional intake during
chemotherapy for advanced colorectal and non-small-cell
lung cancer. J Clin Oncol 1987;5(1):113-24.
5.Bernhardson BM, Tishelman C, Rutqvist LE. Chemosen-
sory changes experienced by patients undergoing cancer
chemotherapy: a qualitative interview study. J Pain Symptom
Manage 2007;34(4):403-12.
6.Sanchez-Lara K, Sosa-Sanchez R, Green-Renner D et al.
Influence of taste disorders on dietary behaviors in cancer
patients under chemotherapy. Nutrition Journal 2010;9:15.
7.Ravasco P, Monteiro-Grillo I, Vidal PM, Camilo ME. Dietary
counseling improves patient outcomes: a prospective,
randomized, controlled trial in colorectal cancer patients
undergoing radiotherapy. J Clin Oncol 2005;23(7):1431-8.
8.Arends J, Bodoky G, Bozzetti F et al. ESPEN guidelines
on enteral nutrition: non-surgical oncology. Clin Nutr
2006;25(2):245-59.
9.Boulton-Jones JR, Lewis J, Jobling JC, Teahon K. Experience
of post-pyloric feeding in seriously ill patients in clinical
practice. Clin Nutr 2004;23(1):35-41.
10.Bozzetti F, Cozzaglio L, Gavazzi C et al. Nutritional
support in patients with cancer of the esophagus: impact
on nutritional status, patient compliance to therapy, and
survival. Tumori 1998;84(6):681-6.
11.Tandon SP, Gupta SC, Sinha SN, Naithani YP. Nutritional
support as an adjunct therapy of advanced cancer patients.
Indian J Med Res 1984;80:180-8.
12.Duerksen DR, Ting E, Thomson P et al. Is there a role
for TPN in terminally ill patients with bowel obstruction?
Nutrition 2004;20(9):760-3.
13.Shang E, Weiss C, Post S, Kaehler G. The influence of
early supplementation of parenteral nutrition on quality of
life and body composition in patients with advanced cancer.
JPEN J Parenter Enteral Nutr 2006;30(3):222-30.
14.Bozzetti F, Cozzaglio L, Biganzoli E et al. Quality of life
and length of survival in advanced cancer patients on home
parenteral nutrition. Clin Nutr 2002;21(4):281-8.
15.Brard L, Weitzen S, Strubel-Lagan SL et al. The effect
of total parenteral nutrition on the survival of terminally ill
ovarian cancer patients. Gynecol Oncol 2006;103(1):176-
80.
16.Bachmann P, Marti-Massoud C, Blanc-Vincent MP
et al. Summary version of the Standards, Options and
Recommendations for palliative or terminal nutrition
in adults with progressive cancer (2001). Br J Cancer
2003;89(Suppl.1):S107-10.
17.Soo I, Gramlich L. Use of parenteral nutrition in
patients with advanced cancer. Appl Physiol Nutr Metab
2008;33(1):102-6.
18.Mercadante S, Casuccio A, Mangione S. Medical
treatment for inoperable malignant bowel obstruction:
a qualitative systematic review. J Pain Symptom Manage
2007;33(2):217-23.
19.Bruera E, Sala R, Rico MA et al. Effects of parenteral
hydration in terminally ill cancer patients: a preliminary
study. J Clin Oncol 2005;23(10):2366-71.
Références bibliographiques
La prescription d’une nutrition parentérale peut cepen-
dant être justifiée si le clinicien estime que le risque
de décès par dénutrition est supérieur au risque de la
progression tumorale. Le cas typique est la carcinose
péritonéale avec occlusion chronique, où la survie
peut être améliorée par la nutrition parentérale (14).
Néanmoins, il manque souvent de critères objectifs
incontestables pour une telle estimation et il n’existe
aucune étude publiée, prospective, randomisée et
comparative ayant stratifié les patients avec et sans
carcinose péritonéale. Dans une étude rétrospective
comparative menée chez 55 patientes atteintes d’un
cancer de l’ovaire et en syndrome obstructif, la nutri-
tion parentérale permettait de gagner 29 jours de
survie. Toutefois, il importe de noter que cet effet
apparemment bénéfique disparaissait après ajuste-
ment sur le traitement chimiothérapique (15).
Dans la majorité des situations, l’anorexie n’est pas
levée par la nutrition parentérale. La faim et la soif
ne sont pas des symptômes constants de la situation
avancée : les patients ne se plaignent ni de faim ni
de soif plus d’une fois sur deux (16). Il existe un
avis d’experts pour éviter de proposer la nutrition
parentérale quand le patient a un indice de Karnofsky
inférieur ou égal à 50 (indice OMS 3 [c’est-à-dire que
le patient passe plus de la moitié du temps assis ou
au lit], et OMS 4 [alitement permanent]), et qu’aucun
projet thérapeutique oncologique, notamment de
chimiothérapie, ne peut plus être envisagé, associé
à une espérance de vie prévisible inférieure à 3 mois
(14, 16). Dans une étude d’observation (38 patients
ayant une nutrition parentérale, dont 84 % présen-
taient un syndrome occlusif), la survie médiane était
de 6 mois quand l’indice de Karnofsky était supérieur
à 50 (médiane 70), versus 3 mois quand il était infé-
rieur ou égal à 50 (17). Une étude de la littérature
montre que la durée de vie moyenne sans support
nutritionnel dans cette situation, avec obstruction
digestive tumorale, est de 48 jours (18). En fin de
vie, une hydratation simple semble suffisante pour
soulager les symptômes (19). Le maintien d’une
qualité de vie acceptable et le traitement sympto-
matique demeurent ici l’objectif premier. Les avis
du patient et de son entourage sont primordiaux
(encadré,p.19).
La synthèse de l’ensemble des recommandations
se trouve sur la gure1 (chimiothérapie à visée
curative) et sur la gure2 (situations palliatives
et palliatives avancées) issues du groupe de travail
Nutrition et cancer de la SFNEP. ■
1
/
5
100%


![Mémo nutrition [à scotcher sur le réfrigérateur]](http://s1.studylibfr.com/store/data/008247290_1-8895597a5435b9765825061d34b3d8ac-300x300.png)