Télécharger l'article au format PDF

L’Encéphale (2010) 36S, D7—D13
Disponible en ligne sur www.sciencedirect.com
journal homepage: www.em-consulte.com/produit/ENCEP
MÉMOIRE ORIGINAL
Vécu subjectif du recontact téléphonique après
tentative de suicide
Patient satisfaction regarding further telephone contact following
attempted suicide
G. Gruata, O. Cottencinb,∗, F. Ducrocqa, S. Duhemc, G. Vaivaa
aService de psychiatrie adulte, CHRU de Lille, Lille, France
bService d’addictologie, université Lille-2, CHRU de Lille, 57, boulevard de Metz, 59037 Lille cedex, France
cCIC, CHRU de Lille, Lille, France
Received 31 December 2008; accepted 7 September 2009
Available online 1 d´
ecembre 2009
MOTS CLÉS
Tentative de suicide ;
Récidive suicidaire ;
Recontact
téléphonique ;
Satisfaction
Résumé La satisfaction des usagers des systèmes de soins est assez peu étudiée dans le
domaine du suicide. Pourtant, dès 1976, certains auteurs retrouvaient un lien entre le risque
suicidaire et un faible niveau de satisfaction envers les soins. À ce jour, seules deux études
consacrées à la prise en charge des patients suicidants comportaient une évaluation de la satis-
faction des patients (retrouvant d’ailleurs un lien fort entre insatisfaction et risque suicidaire).
Au cours de l’étude SYSCALL mesurant l’impact d’un recontact téléphonique systématique sur
la récidive dans les semaines suivant une tentative de suicide, nous avons voulu savoir si cette
procédure ainsi que ses modalités avait été bien acceptée par les patients. Lors du dernier
recontact programmé 13 mois après la tentative de suicide index, nous avons évalué le vécu
des patients face à cette intervention et son impact sur leur devenir au moyen d’un ques-
tionnaire : 54% des patients interrogés ont répondu, 78,9 % d’entre eux considéraient que le
recontact leur avait été bénéfique et 40,4 % estimaient qu’il avait eu une influence sur leur
vie voire pour 29,4 % qu’il leur avait évité une récidive suicidaire ; 94,5 % étaient satisfaits de
son déroulement, mais 20,2 % auraient aimé être recontactés par un médecin connu. Enfin,
la majorité des patients recontactés étaient satisfaits du moment choisi. Le recontact télé-
phonique, malgré sa nature intrusive et inhabituelle, a été bien accepté par les patients, ainsi
que ses modalités. Nous pensons que le recueil de l’opinion des patients est aussi à développer
en tant qu’outil thérapeutique dans la prise en charge des suicidants.
© L’Encéphale, Paris, 2009.
∗Auteur correspondant.
E-mail address: [email protected] (O. Cottencin).
0013-7006/$ — see front matter © L’Encéphale, Paris, 2009.
doi:10.1016/j.encep.2009.10.009

D8 G. Gruat et al.
KEYWORDS
Telephone contact;
Suicide attempt;
Recurrence of suicide
attempt;
Client satisfaction
Summary At a time when increasing importance is given to providing satisfaction to the users
of health services, it is surprising that this concept has hardly ever been examined in the field of
suicide. Although suicide (prevention and management) is an important part of public health,
there seems to be little interest in finding out patients’ opinions about the healthcare services
which are offered to them. Back in 1976, some authors found a link between the risk of suicide
and a low level of satisfaction of healthcare. To date, only two studies looking at management of
suicidal patients have included an assessment of patient satisfaction (a strong link between dis-
satisfaction and suicidal risk was found). During the SYSCALL study, which measured the impact
of systematic recontacting by telephone on recurrence of suicide, in the weeks following a
suicide attempt, we aimed to find out if this procedure and its methods were well-accepted by
the patients. When the patients were first recontacted, 13 months after the suicide attempt,
and included in our study, we assessed by means of a questionnaire, their experience of being
faced with this intervention, and its impact on their future. Of the 605 patients included, 312
were put into the control group, 147 were recontacted at the end of the first month, and 146 at
the end of the third month. The rate of repeat suicide attempts in the year following the initial
attempt, was significantly lower in the group that was recontacted after one month, than in
the control group [12% against 22%; P= 0.03]. It would therefore seem that systematic recon-
tacting by telephone one month after attempted suicide may have contributed in reducing the
risk of an early repeat suicide attempt. Of the 482 patients whom we managed to contact by
13 months, 254 had filled out the questionnaire about their subjective experience, in writing or
by telephone, this making a response rate of 52.7%. Amongst the patients who replied, female
patients are over-represented with more of them being recontacted than males, but no dif-
ference was found in the psychiatric symptomatology observed when they were assessed and
included in the study. On the other hand, we found a higher incidence of mood disorders and
suicidal risk in those who were examined at the final assessment at 13 months. A large majority
(78.9%) of the patients who were recontacted, considered recontacting as beneficial, 40.4%
considered that it had influenced their lives, and 29.4% thought that recontacting had con-
tributed to avoiding them making a further suicide attempt. Out of the patients recontacted,
94.5% had appreciated the person that had recontacted them, and only 8.3% had been disturbed
at being recontacted by a different doctor than the one whom they had met in the Emergency
department. A majority of them (54.1%) considered that telephoning was the most appropriate
method for recontacting, but of those who were not convinced of being recontacted by tele-
phone, 89.5% of them thought that consultation was the best alternative. Finally, around a third
of patients would have preferred being recontacted earlier. On closer examination of the 10
recontacted patients who were dissatisfied by being recontacted, we did not find any elements
to characterize them, except for a previous history of more suicide attempts in their family.
Finally, a majority of the dissatisfied patients would have preferred being notified in advance
of the time of recontacting, and half of them thought that recontacting was too late, but they
were not disturbed by being contacted by a different doctor. Telephone recontacting and its
methods were surprisingly well-accepted by the patients, even though it is intrusive in nature
and unusual in France. We think that despite the inevitable bias that is linked to it, the opinion
of patients should be sought and developed in the management of patients who have attempted
suicide and in the treatment of the suicidal crisis in general. Even though patients’ satisfaction
rates may improve the quality of treatment, we should bear in mind that listening to, noting
down and examining patients’ opinions and words, is in itself a useful factor for patients in
their quest for improving their health.
© L’Encéphale, Paris, 2009.
Introduction
À l’heure où une importance grandissante est accordée à la
satisfaction des usagers des systèmes de soins, il est assez
surprenant que dans le domaine du suicide, cette notion
soit si peu explorée. Pourtant, le suicide fait partie des
enjeux importants de santé publique et, dans le domaine
de sa prévention, la prise en charge des patients après une
tentative de suicide est un sujet de recherche prioritaire.
Pourtant, dès 1976, Richman et Charles retrouvaient un lien
entre le risque suicidaire et un faible niveau de satisfac-
tion envers les soins [15], ce que confirmera Lebow dans sa
revue de littérature sur la satisfaction en psychiatrie [10].
Parmi les nombreuses études consacrées à la prise en charge
des patients après tentative de suicide, seules quelques-
unes ont étudié le recueil du point de vue des patients dont
deux portaient sur les systèmes d’intervention au décours
d’un geste suicidaire [2,6]. La première retrouvait un indice
moyen de satisfaction plus élevé chez les patients ayant
bénéficié de séances de psychothérapie à leur domicile que
chez ceux ayant eu la prise en charge usuelle [6]. La sec-
onde évaluait une prise en charge psychosociale réalisée
par un intervenant spécialisé dans le suicide et retrouvait
parmi les répondeurs 76 % de satisfaction avec un lien net

Vécu subjectif du recontact téléphonique après tentative de suicide D9
entre insatisfaction et risque suicidaire [2]. Plusieurs fac-
teurs peuvent expliquer ce manque de données : la réticence
des soignants à se sentir jugés, les biais inhérents au recueil
de l’opinion des patients, le manque de concertation sur le
terme «satisfaction ». Pourtant, pour Sitzia et Wood, trois
dimensions au moins sont à prendre en compte : la capacité
des soignants à créer une relation de soins confortable, les
changements ressentis par les patients et leurs attentes et
enfin, la pertinence des soins par rapport à celles-ci [17].
Or les patients suicidaires se reconnaissent plus de besoins
que les autres patients [14] et sont plus nombreux à con-
sidérer que leurs attentes n’ont pas été remplies par la
prise en charge [4,14], d’où l’importance et la nécessité de
s’intéresser à leur point de vue sur les soins.
Dans le Nord—Pas-de-Calais, l’impact sur les récidives
d’un recontact téléphonique systématique, dans les
semaines suivant une tentative de suicide, a été évalué
dans le cadre de l’étude SYSCALL. Nous ne reprendrons
pas en détail les résultats de cette étude [18], mais nous
intéresserons au vécu des patients face à cette interven-
tion inhabituelle et à leur évaluation de l’impact d’une telle
méthode.
L’étude SYSCALL
SYSCALL [18] est une étude multicentrique randomisée
réalisée dans 13 centres d’urgences du Nord—Pas-de-Calais :
605 patients, se présentant aux urgences après une tenta-
tive de suicide par intoxication médicamenteuse volontaire
et pour qui un psychiatre jugeait qu’une hospitalisation
n’était pas nécessaire, ont été inclus dans l’étude et
randomisés en deux groupes. Les patients du groupe témoin
bénéficiaient de la prise en charge usuelle et n’étaient
joints qu’après 13 mois. Les patients du groupe intervention
étaient recontactés par téléphone soit à un mois soit à trois
mois de leur sortie des urgences. La randomisation était
stratifiée sur le sexe et le pourcentage de multirécidivistes
(plus de quatre tentatives de suicide dans les trois ans
passés). L’objectif principal de l’étude était de mesurer
l’influence d’un recontact téléphonique systématique après
une tentative de suicide sur la récidive précoce. Au cours de
cet entretien téléphonique les investigateurs s’assuraient de
la pertinence des modalités de suivi prévues aux urgences,
de les réajuster si nécessaire, rappelaient les numéros de
téléphone «ressources »et évaluaient l’état psychique du
patient avec la possibilité d’une prise en charge rapide en
cas de souffrance psychique ou de risque suicidaire. Au
13emois de l’étude, une évaluation finale était réalisée pour
l’ensemble de la cohorte au cours de laquelle étaient éval-
ués l’existence de troubles psychiatriques, les données sur
le devenir, les récidives éventuelles et le parcours de soins.
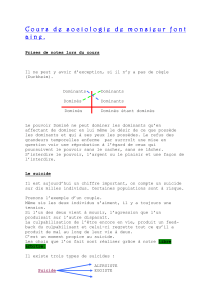
Sur les 605 patients inclus, 312 ont formé le groupe témoin,
147 ont été recontactés à la fin du premier mois et 146 à
la fin du troisième. Le taux de récidives suicidaires dans
l’année suivant le geste suicidaire dans le groupe recontacté
à un mois était significativement plus faible que dans le
groupe témoin (12 % vs 22 % ; p = 0,03), mais non significatif
dans le groupe à trois mois (17 % vs 22 % ; p= 0,27). Ainsi, il
semblait donc qu’un recontact téléphonique systématique,
un mois après une tentative de suicide, ait contribué à
diminuer le risque de récidive suicidaire précoce (Fig. 1).
Objectif
Parce que cette mesure inhabituelle en France, nous parais-
sait intrusive, nous avons voulu connaître le vécu des
patients dans le déroulement de la procédure et l’impact
qu’ils avaient attribué à ce recontact. Dans l’objectif
Figure 1 Description de l’étude SYSCALL avec les résultats significatifs montrant que le recontact téléphonique précoce (à un
mois) diminue significativement le risque de récidive suicidaire à un an en comparaison des autres groupes.

D10 G. Gruat et al.
Tableau 1 Comparaison des patients ayant répondu au questionnaire de vécu subjectif et des patients n’ayant pas répondu.
Questionnaires remplis Oui Non p
n= 254 (%) n= 345 (%)
Multirécidivistes 11,8 7,2 0,056
Recontactés 42,9 26,7 < 0,0001
Femmes 78,7 67,2 0,002
Présence à visite finale de... n= 254 (%) n= 228 (%)
Trouble de l’humeur
Trouble anxieux
Risque suicidaire
35,3
56,4
20,7
23,2
51,2
11
0,009
0,301
0,01
d’évaluer l’acceptation du recontact et de ses modalités,
nous avons proposé aux patients de répondre à un question-
naire de satisfaction.
Patients et méthode
Deux questionnaires distincts ont été élaborés : l’un pour
le groupe témoin, l’autre pour les patients recontac-
tés. Le questionnaire était joint au courrier annonc¸ant le
rendez-vous téléphonique pour l’évaluation finale. Si le
questionnaire n’avait pas été retourné, les patients pou-
vaient y répondre lors de l’évaluation téléphonique finale.
Les deux questionnaires abordaient des questions sur la prise
en charge après leur tentative de suicide, les attentes et les
a priori quant au recontact. Pour les patients recontactés,
nous avons ajouté des questions sur l’impact du recontact
sur leur vie et demandé leur appréciation des modalités du
recontact.
Résultats
Parmi les 482 patients ayant pu être joints à 13 mois, 254 ont
rempli le questionnaire de vécu subjectif (taux de réponses
de 52,7 % sans différence entre les trois groupes) (Tableau 1).
Nous retrouvions chez les répondeurs une surreprésentation
féminine, une plus grande proportion de patients recontac-
tés et une plus grande fréquence de troubles de l’humeur et
de risque suicidaire chez les répondeurs à l’évaluation finale
du 13emois.
Vécu subjectif du recontact
Cent neuf patients recontactés (57 à un mois et 52 à trois
mois) ont donc répondu au questionnaire de vécu subjec-
tif (soit un taux de réponse de 37,2 %). La grande majorité
(78,9 %) d’entre eux considérait le recontact bénéfique. Ils
étaient 40,4 % à considérer qu’il avait eu une influence sur
leur vie et 29,4 % des patients estimaient que le recontact
avait contribué à leur éviter une nouvelle tentative de sui-
cide. Nous ne notions aucune différence significative entre
les deux groupes (Tableau 2).
Modalités du recontact
Parmi les patients recontactés, 94,5 % déclaraient avoir été
bien rec¸us par la personne chargée du recontact et le fait
qu’il ait été effectué par un médecin différent de celui ren-
contré aux urgences n’avait gêné que 8,3 % des patients
même si 20,2 % auraient préféré être recontactés par un
médecin connu. La majorité d’entre eux (54,1 %) consid-
Tableau 2 Vécu subjectif des patients recontactés.
Groupe recontactés M1 M3 (n= 109) Oui (%) Non (%) NSP (%)
Le recontact a-t-il été bénéfique ? 78,9 9,2 11,9
Avez-vous été bien rec¸u(e) par le recontacteur ? 94,5 1,8 3,7
Était-ce une gêne que ce ne soit pas le médecin des Urgences ? 8,3 89,9 1,8
Auriez-vous préféré un contact avec un médecin connu ? 20,2 74,3 5,5
Le téléphone est-il une procédure appropriée ? 54,1 29,4 16,5
Avec 89,5 % proposant comme alternative un contact direct
Le recontact a-t-il eu une influence sur votre vie ? 40,4 49,5 10,1
Le recontact a-t-il permis d’éviter récidive suicidaire ? 29,4 56 14,7
Souhaitiez-vous un recontact plus tôt ? 29,4 45,0 25,7
Souhaitiez-vous un recontact plus tard ? 4,6 52,3 43,1
À l’annonce du recontact, étiez-vous ennuyé(e) ? 14,7 62,4 22,9
À l’annonce du recontact, étiez-vous satisfait(e) ? 76,1 9,2 14,7
Groupe M1 : recontactés à un mois ; groupe M3 : recontactés à trois mois ; NSP : ne se prononce pas.

Vécu subjectif du recontact téléphonique après tentative de suicide D11
Tableau 3 Description des patients en fonction de leur satisfaction par rapport au recontact téléphonique.
Dans votre cas, pensez-vous que le recontact a été bénéfique ? Non(n= 10) (%) Oui(n= 86) (%) p
Recontactés à un mois ou à trois mois
ATCD familiaux de TS 71,4 26,3 0,024
Trouble de l’humeur à la visite finale 55,6 23,8 0,055
Le recontact devrait concerner tout le monde 60 93 0,002
Importance d’un recours téléphonique d’urgence 60 90,7 0,007
Gêne d’un recontact par un médecin inconnu 30 3,5 0,01
Tableau 4 Comparaison du vécu subjectif des primosuicidants et des récidivistes.
Primosuicidants Récidivistes p
Total des répondeurs au 13emois n = 129 n= 125
Jugent positif que les urgences contactent leur médecin 55,8 % 68 % 0,012
Groupe recontact à 1 mois et à 3 mois n = 54 (%) n= 55 (%)
Ressentent un bénéfice du recontact 79,6 78,2 ns
Ressentent un impact positif du recontact 38,9 41,8 ns
Auraient voulu un recontact plus précoce 16,7 41,8 0,013
Groupe témoin (non recontacté) n = 75 (%) n= 70 (%)
Pensent que recontact aurait été bénéfique 48 71,4 0,010
Pensent que recontact aurait entraîné un changement 26,7 41,4 0,015
éraient le téléphone comme la méthode la plus appropriée,
mais l’alternative choisie par 89,5 % des patients non con-
vaincus était la consultation. Enfin, la majorité d’entre eux
(quel que soit le groupe) considéraient le moment du recon-
tact adapté (groupe M1 [61,4 %] vs groupe M3 [80,8 %] ;
p= 0,079) (Tableau 2).
Quelle insatisfaction ?
Dix patients recontactés (cinq du groupe M1 et cinq du
groupe M3) ont déclaré que le recontact ne leur avait
été d’aucun bénéfice. Sur le plan sociodémographique
ou psychopathologique à l’évaluation initiale, aucun élé-
ment n’était caractéristique de cette population, sinon une
fréquence plus importante d’antécédents familiaux de ten-
tatives de suicide. En revanche, ils présentaient une plus
grande fréquence de troubles de l’humeur et de troubles
anxieux, sans qu’il n’y ait de différence statistiquement
significative. Enfin, leur appréciation sur les modalités du
recontact différait selon la satisfaction. Ainsi, la majorité
des patients insatisfaits auraient souhaités être prévenus du
moment du recontact et la moitié d’entre eux ont consid-
éré que le recontact avait été trop tardif, sans pour autant
avoir été gênés par le fait d’être contactés par un nouvel
interlocuteur (Tableau 3).
Le cas des primosuicidants
Cent vingt-neuf patients ont été inclus après un premier
geste suicidaire et 54 d’entre eux ont été recontactés.
Ces patients semblaient avoir moins d’attente par rapport
aux soins puisqu’ils étaient moins nombreux à consid-
érer comme positif le fait de maintenir un lien entre les
urgences et leur médecin traitant, et étaient moins nom-
breux à considérer que le recontact téléphonique aurait
dû concerner tous les patients suicidants. Les primosuici-
dants du groupe témoin (n= 75) semblaient plus sceptiques
sur le recontact que les récidivistes étant moins nom-
breux à considérer qu’il aurait pu induire un changement
ou leur être bénéfique. À l’inverse, s’ils avaient bénéfi-
cié du recontact, ils lui accordaient autant de bénéfice et
lui imputaient autant d’influence que les autres patients
(Tableau 4).
Discussion
L’objectif principal de notre étude était d’évaluer le vécu
des patients face à une procédure thérapeutique inhab-
ituelle en France : le recontact téléphonique systématique
après une tentative de suicide.
Notre premier constat était qu’une très grande majorité
des patients considérait ce recontact bénéfique et la procé-
dure téléphonique adaptée. Un résultat cohérent avec la
littérature qui nous place dans la moyenne de satisfac-
tion des soins psychiatriques ambulatoires classiques [1,10].
Ainsi, malgré notre culture «latine », nous pouvons con-
stater que cette procédure n’a pas déstabilisé les patients.
Par ailleurs, nous ne sommes pas étonnés de constater que
les patients considéraient le contact direct (consultation)
comme une bonne alternative au contact téléphonique.
Soulignons cependant que c’est justement l’échec des
procédures classiques de suivi des patients qui nous a con-
duits à élaborer le recontact téléphonique en raison de
la faible adhésion aux soins post-urgence (puisque seuls
40 % des patients se rendent au rendez-vous de suivi [3]).
Ainsi, le recontact téléphonique ne doit pas être confondu
 6
7
6
7
1
/
7
100%