Physiopathologie du paludisme à Plasmodium falciparum

V. Laurent
222 | La Lettre de l’Infectiologue • Tome XXVII - n° 6 - novembre-décembre 2012
DOSSIER THÉMATIQUE
Paludisme
Physiopathologie
du paludisme à Plasmodium
falciparum : principaux
mécanismes et avancées
récentes
Pathophysiology of Plasmodium falciparum malaria:
main pathways and recent progress
V. Laurent1, P. Buffet2-5, S. Jauréguiberry3, 4, 6, F. Bruneel1
1 Service de réanimation médico-
chirurgicale, centre hospitalier de
Versailles.
2 Service de parasitologie-mycologie,
hôpital de la Pitié-Salpêtrière, Paris.
3 Centre national de référence du
paludisme pour la France métro-
politaine.
4
Inserm-université Pierre-et-Marie-
Curie, UMRs945.
5 Institut Pasteur de Paris.
6 Maladies infectieuses et médecine
tropicale, hôpital de la Pitié-Salpê-
trière, Paris.
M
algré de nombreux travaux récents fonda-
mentaux et expérimentaux, la physiopa-
thologie du paludisme n’est pas encore
parfaitement élucidée. Cela s’explique par son
caractère complexe et plurifactoriel. Les principaux
mécanismes impliquent l’hôte et le parasite dans
des interactions nombreuses et souvent syner-
giques. Nous rapportons ici une vue d’ensemble de la
physiopathologie du paludisme grave à Plasmodium
falciparum, en détaillant les principaux mécanismes
incriminés (cellulaires, immunologiques, humoraux),
ainsi que certaines données récentes (rôle de la rate,
microparticules).
La séquestration des hématies
parasitées
La séquestration peut schématiquement se
décomposer en 3 mécanismes : la cytoadhérence,
la formation de rosettes et l’autoagglutination. La
cytoadhérence est le mécanisme prépondérant et
correspond à l’adhérence des hématies parasitées
(HP) aux cellules endothéliales. La capacité des
HP à lier des hématies non parasitées conduit à la
formation de rosettes (rosetting). L’autoagglutina-
tion correspond à l’adhérence entre plusieurs HP,
phénomène secondaire et probablement favorisé
par les plaquettes.
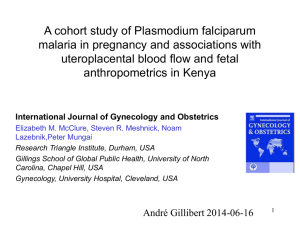
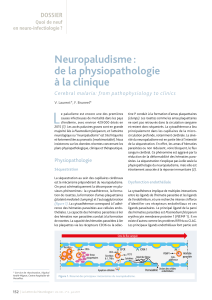
La cytoadhérence a lieu principalement dans les
capillaires de la microcirculation profonde, parti-
culièrement bien étudiée au niveau cérébral
(figure 1). Elle se fait au niveau de protubérances
électrodenses (knobs) visualisées en microscopie
électronique à la surface de la membrane des HP,
en regard de la zone de contact avec la cellule endo-
théliale. Au niveau moléculaire, la cytoadhérence
implique de multiples interactions entre les ligands
de l’hématie et les ligands de l’endothélium (1).
Les principaux ligands de la paroi des HP sont P.
falciparum Erythrocyte Membrane Proteine-1, -2
et -3 (PfEMP-1, -2 et -3) et P. falciparum Histidine
Rich Protein-1 et -2 (Pf HRP-1 et -2). Les protéines
PfHRP-1, PfEMP-2, PfEMP-3 ne sont pas exprimées
à la surface de l’HP, mais localisées à la face interne
de sa membrane, où elles interagissent entre elles
et avec les protéines du squelette membranaire.
En revanche, PfEMP-1 est exprimée en surface et
semble être la plus importante (figure 1). P. falci-
parum a environ 60 gènes var encodant une protéine
PfEMP-1 probablement porteuse d’antigènes diffé-
rents capables d’avoir des propriétés de cytoadhé-
rence variables. Parmi les autres ligands d’origine
parasitaire, on retrouve également des membres des
familles des Repetitive Interspersed Family (RIFINS)
et des Cytoadherence Linked Asexual Gene (CLAG).
Le principal ligand de l’HP, d’origine érythrocytaire
et non parasitaire, est une glycoprotéine de surface,

Cellule endothéliale
Globule rouge parasité
PfEMP 1
Globule rouge
Globule blanc
Plaquette
Microparticules
Neurone
Cytokines
Séquestration des globules rouges parasités
et non parasités, et des plaquettes
Relargage de citokines pro-
et anti-inflammatoires
Relargage de microparticules
Lésions des cellules
endothéliales
Apoptose cellulaire
Sens du flux sanguin
Figure 1. Schéma résumant les mécanismes du paludisme grave à Plasmodium falciparum au niveau des capillaires
cérébraux.
La Lettre de l’Infectiologue • Tome XXVII - n° 6 - novembre-décembre 2012 | 223
Points forts
»
La physiopathologie du paludisme est complexe, encore imparfaitement élucidée, et fait l’objet de très
nombreux travaux de recherche.
»
Le mécanisme prépondérant est la séquestration qui correspond aux interactions entre les hématies
parasitées et l’endothélium des vaisseaux capillaires.
»
P. falciparum
stimule aussi la réaction inflammatoire et l’immunité innée et adaptative.
»Les rôles des plaquettes et des microparticules cellulaires ont été plus récemment étudiés.
»
La rate participe à la réaction immunologique et a un rôle central et original de filtration, de rétention,
de destruction et d’épépinage des hématies parasitées.
Mots-clés
Paludisme
Physiopathologie
Cytoadhérence
Cytokine
Rate
Pitting
Highlights
»
The pathophysiology of
malaria is complex; still imper-
fectly known, it is a major field
of research.
»
The main pathway is cytoad-
herence between parasitized
red blood cells and endothelial
cells of the capillaries of the
host’s organs.
»
P. falciparum
also strongly
induces both inflammatory and
immunologic responses.
»
The participation of platelets
and microparticles has recently
been described.
»
The spleen plays a part in
the immunologic response, but
morever it has a very specific
part in filtration, retention,
destruction and pitting of the
parasitized red blood cells.
Keywords
Malaria
Pathophysiology
Cytoadherence
Cytokine
Spleen
Pitting
la bande 3 qui, modifiée par le parasite, aurait un
rôle dans la séquestration (2).
Les principaux ligands de la surface endothéliale
font partie de la superfamille des immunoglobulines
(ICAM-1, VCAM-1, PECAM-1), des glycoprotéines
(CD-36, sélectine E, thrombospondine, sélectine P)
ou des glyco-aminoglycanes comme le chondroïtine
sulfate A (CSA).
L’intensité de la séquestration est au moins en partie
corrélée avec la gravité du paludisme. Les amas
d’hématies, parasitées ou non, par cytoadhérence,
rosetting et auto-agglutination, réduisent le flux
sanguin au niveau des microvaisseaux profonds,
principalement cérébraux (figure 1). Ce phénomène
d’altération du flux est aggravé par la réduction de
la déformabilité des HP (3). Même si les nécroses
tissulaires sont rares, et que les signes, notamment
neurologiques, peuvent être réversibles, l’hypoxémie
et la perfusion tissulaire inadéquates, aggravées par
l’anémie et l’hypoglycémie, sont responsables de
lésions cérébrales. La séquestration parasitaire au
sein du réseau vasculaire est difficile à quantifier. En
effet, la parasitémie ne représente que la biomasse
parasitaire circulante. Le taux plasmatique d’HRP-2
semble être un meilleur reflet de la biomasse para-
sitaire totale (circulante et séquestrée) [4]. Au final,
les HP séquestrées dans les capillaires profonds,
agglutinant des hématies saines et des plaquettes,
se trouvent protégées pour progresser dans le cycle
parasitaire, mais aussi pour produire et stimuler une
variété de molécules bioactives qui participent au
processus pathologique.
La réponse humorale
Les cytokines
La réponse immunitaire aux agents infectieux est
principalement initiée par l’interaction des Pathogen

224 | La Lettre de l’Infectiologue • Tome XXVII - n° 6 - novembre-décembre 2012
DOSSIER THÉMATIQUE
Paludisme
Associated Molecular Patterns (PAMP) avec les récep-
teurs exprimés par les cellules de l’hôte. Beaucoup
d’études impliquent la principale toxine de P. falci-
parum, le glycosylphosphatidylinositol (GPI), en
tant que PAMP du parasite. Le GPI purifié induit
l’expression de nombreux gènes impliqués dans la
pathogenèse du paludisme, par exemple les gènes
qui codent pour les cytokines pro-inflammatoires,
comme le Tumor Necrosis Factor (TNF), l’interleu-
kine 1 (IL-1) et différentes molécules d’adhésion qui
sont exprimées à la surface de l’endothélium (5). Ce
dernier mécanisme illustre bien la synergie entre
réaction humorale et cytoadhérence (6). Le rôle des
cytokines dans la pathogénie n’est pas connu avec
précision. Le TNF est la cytokine pro-inflammatoire
la plus étudiée. La sécrétion de TNF, cytokine pyro-
gène essentiellement produite par les macrophages
activés, serait secondaire à la rupture paroxystique
des schizontes qui libèrent les mérozoïtes, expliquant
ainsi les importantes variations des taux circulants de
cette cytokine. Le TNF est surexprimé près des zones
de séquestration intense ; il augmente l’expression
d’ICAM-1 à la surface des cellules endothéliales,
favorisant ainsi la cytoadhésion des HP (7). Au stade
précoce de la maladie, le TNF pourrait jouer un rôle
protecteur, alors qu’il jouerait le rôle inverse au stade
tardif (8). Il est aussi impliqué dans la régulation de
la transmission sympathique ; il stimule la synthèse
de l’oxyde nitrique (NO), et pourrait participer ainsi
aux symptômes du neuropaludisme.
Mécanismes immunitaires
L’infection par P. falciparum stimule la réponse
immunitaire de l’hôte. Ces réponses mettent en
jeu le système immunitaire inné aussi bien que le
système adaptatif. L’immunité innée se mobilise
dès les premières heures de l’infection, et l’immu-
nité adaptative est opérationnelle dans les 10 jours
suivants. Les neutrophiles, les monocytes et les
cellules NK (Natural Killer) semblent jouer un rôle
prépondérant dans l’immunité innée observée au
cours de la phase précoce du paludisme. Le taux des
cellules NK augmente tant qu’elles sont capables
de détruire in vitro les globules rouges parasités
par P. falciparum (9). Elles sont aussi de puissantes
productrices de cytokines telles que l’IFNγ.
Les cytokines libérées lors de l’activation endothéliale
peuvent recruter les monocytes et activer les neutro-
philes (figure 1, p. 223). Les monocytes recrutés
peuvent ensuite se différencier en macrophages, qui
se mobilisent dans les microvaisseaux. Les macro-
phages peuvent aussi être activés directement par le
GPI, comme pourrait le faire une endotoxine bacté-
rienne. Ce processus est accru par l’IFNγ. Les macro-
phages activés produisent plus de chémokines, ce
qui amplifie l’infiltration cellulaire, la séquestration
des HP et le relargage de microparticules.
C’est seulement après plusieurs cycles que les
lymphocytes T entrent en jeu, libérant à leur tour des
cytokines et des chémokines pouvant être respon-
sables de lésions (10).
Rôle des plaquettes
et des microparticules
Plaquettes
Le rôle des plaquettes au cours du paludisme grave
fait l’objet de plus en plus de publications (figure 1,
p. 223). Il y a de nombreuses voies possibles par
lesquelles les plaquettes pourraient affecter la
fonction et la viabilité des cellules endothéliales et
promouvoir l’adhésion des leucocytes.
Les plaquettes, avec d’autres types de cellules,
peuvent moduler l’expression des molécules d’adhé-
sion (ICAM-1) et la production de cytokines comme
l’IL-6 par les cellules endothéliales via le relargage
d’IL-1. Ainsi, elles peuvent améliorer l’adhésion des
leucocytes aux cellules endothéliales et augmenter la
susceptibilité des cellules endothéliales au TNF. Ces
mécanismes peuvent participer à la séquestration
et favoriser les hémorragies constatées au cours du
neuropaludisme. Ensuite, les microparticules dérivées
des plaquettes modulent le métabolisme endothélial
et augmentent l’adhérence entre les plaquettes, les
leucocytes et les cellules endothéliales par une régula-
tion positive de l’expression des molécules d’adhésion
et des intégrines comme ICAM-1 et le récepteur aux
macrophages 1 (11). Les plaquettes peuvent aussi
altérer les cellules endothéliales en potentialisant la
production de cytokines par les leucocytes. Elles sont
également capables de moduler l’interaction avec les
HP par le biais de leur antigène de surface CD-36 et
de participer ainsi à l’occlusion des capillaires. Enfin,
les plaquettes jouent le rôle d’intermédiaire dans
l’agglutination des HP (12).
Microparticules
Les microparticules sont désormais considérées
comme jouant un rôle important dans le dévelop-
pement du neuropaludisme (figure 1, p. 223). Ce
Physiopathologie dupaludisme à
Plasmodium falciparum
:
principaux mécanismes et avancées récentes

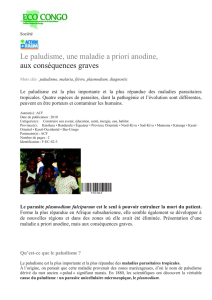
MF
MF/CD
Débit artériel
entrant
Circulation rapide “fermée”
Zone périfolliculaire (ZPF)
Interactions ligand – récepteur
entre globules rouges et macrophages
Circulation “ouverte”
et lente
Cordons de la pulpe rouge
Rétention de globules rouges rigides
Pitting de corps figurés intraérythrocytaires
Modifications des GR induites par la stase
Phagocytose/recyclage du fer
Instauration d’une réponse spécifique
d’antigène Débit veineux
sortant
1. Préfiltration
2. Filtration stricto sensu
3. Post-filtration
Court-circuit
ZPF - sinus
Sinus
Cellules
endothéliales
Fibres basales
Veinule post-
sinusale
Figure 2. Structure schématique et organisation de l’unité fonctionnelle filtrante splénique :
le “splénon”, terme forgé par analogie avec le “néphron”, unité fonctionnelle filtrante
rénale. La microcirculation splénique comporte 2 cheminements parallèles : la circulation
rapide et fermée et la circulation ouverte et lente, par où passent respectivement 90 %
et 10 % du débit sanguin splénique. La circulation dans les cordons de Billroth (pulpe
rouge) est dite “ouverte” car se produisant dans des espaces dépourvus d’endothélium.
La circulation y est 20 fois plus lente que dans la circulation rapide, ce qui facilite les inter-
actions étroites avec les macrophages (MF) qui représentent environ la moitié du volume
des cordons (étape de “préfiltration” reposant sur des interactions “conventionnelles” de
type ligand-récepteur). Le retour à la circulation générale impose la traversée de la paroi
sinusale qui sollicite de façon rigoureuse la déformabilité érythrocytaire (étape de filtration
stricto sensu). Pour éviter la saturation du filtre splénique, les globules rouges retenus
aux étapes précédentes doivent être éliminés. Cette élimination se fait probablement
par phagocytose (MF ou cellules dendritiques [CD]), qui permet le recyclage du fer et
l’instauration d’une réponse spécifique d’antigène. Cette troisième étape de postfiltration
fait le lien entre les étapes innées de rétention érythrocytaire et l’immunité adaptative.
La Lettre de l’Infectiologue • Tome XXVII - n° 6 - novembre-décembre 2012 | 225
DOSSIER THÉMATIQUE
sont des vésicules microscopiques (de 0,2 à 1 μm)
dérivées des membranes cellulaires de différentes
cellules, extériorisées durant un phénomène physio-
logique connu sous le nom de “vésiculation”. Les
microparticules qui en découlent ont une bicouche
lipidique parsemée de phosphatidylsérine, tandis
que leur membrane externe exprime les antigènes
de leur cellule d’origine (13).
Dans les conditions physiologiques normales, les
microparticules dérivent de tous les types cellulaires et
principalement des plaquettes, des érythrocytes, des
leucocytes et des cellules endothéliales. Les amino-
phospholipides exprimés à leur surface permettent
des sites d’attache pour les facteurs de coagulation
(IXa, VIII, Va, prothrombinase et la ténase), ce qui
facilite les interactions de cellule à cellule, la signa-
lisation, la coagulation et l’inflammation (14)..
Le rôle des microparticules dans la pathogenèse
de la maladie est suggéré par les modèles expé-
rimentaux de neuropaludisme, où les taux de MP
sont augmentés dans le plasma au moment de l’at-
teinte cérébrale. A contrario, l’absence de surpro-
duction de microparticules est associée à l’absence
de neuropaludisme, à parasitémie égale (15). Enfin,
chez des enfants atteints de neuropaludisme, le
taux de microparticules d’origine plaquettaire est
corrélé à la profondeur et à la durée du coma (16).
Rôle de la rate
dans la physiopathologie
du paludisme
La grande fréquence de la splénomégalie en zone d’en-
démie palustre (17), la survenue de ruptures spléniques
pathologiques au cours ou au décours immédiat d’accès
palustres (18) et, surtout, la gravité plus fréquente et
plus marquée des premiers accès chez les patients
splénectomisés (19) illustrent le rôle central de la rate
dans la physiopathologie du paludisme. Les stades
pathogènes de P. falciparum se développent dans les
globules rouges et en modifient les propriétés (20). Il
est logique que l’organe ayant pour fonction (entre
autres) de contrôler la qualité des globules rouges (21)
influence le cours de l’infection. Lors de leur passage
par la rate, les globules rouges entrent en contact étroit
avec les macrophages de la pulpe rouge et sont alors
phagocytés si leur surface est altérée ou opsonisée
(figure 2) [21, 22]. Les globules rouges franchissant
cette première étape, traversent ensuite une structure
microanatomique spécifique – la paroi sinusale – qui
contrôle leurs propriétés mécaniques et retient ceux
qui sont insuffisamment déformables (figure 2) [21,
23, 24]. De nouveaux outils tels que la perfusion de rate
humaine ex vivo (25) et la filtration sur micro sphères
(microfiltration) [26] ont été développés pour explorer
expérimentalement ces phénomènes physiologiques.
Ces outils ont montré la rétention splénique d’une
partie des globules rouges parasités par P. falciparum,
tant au stade asexué responsable des symptômes du
paludisme (27) qu’au stade sexué impliqué dans la
transmission (gamétocytes) [28]. La topographie de
cette rétention et d’autres mesures biophysiques ont
montré qu’une partie des formes jeunes, normalement
circulantes, sont retenues de façon mécanique dans
la rate (27). Ce processus inné réduirait la biomasse
susceptible de cytoadhérer quelques heures plus tard
dans les capillaires des organes cibles (cerveau, rein)
et capable de poursuivre la multiplication (29). L’âge
de l’hôte a – indépendamment du niveau d’endémie
– une influence sur la gravité des premiers accès (30).

226 | La Lettre de l’Infectiologue • Tome XXVII - n° 6 - novembre-décembre 2012
DOSSIER THÉMATIQUE
Paludisme
Physiopathologie dupaludisme à
Plasmodium falciparum
:
principaux mécanismes et avancées récentes
Le ou les mécanismes par lesquels le jeune âge réduit
le risque de paludisme grave sont actuellement
inconnus (19). Il est possible que l’intensité variable
de cette rétention splénique détermine en partie
l’évolution ou bien vers l’anémie palustre grave du
nourrisson (rétention forte, évolution subaiguë, charge
parasitaire moyenne), ou bien vers le neuropaludisme
du jeune enfant (faible rétention, évolution rapide,
forte charge parasitaire) [29]. La rétention mécanique
est très probablement un déterminant important de
la circulation des gamétocytes et donc de la trans-
mission (28). L’expression de la famille multigénique
stevor est associée à ces modifications phénotypiques
(28, 31).
La rate joue aussi un rôle important dans la clairance
parasitaire sous traitement antipaludique, particu-
lièrement lorsque le traitement comporte un dérivé
de l’artémisinine (artésunate, dihydroartémisinine)
[32]. Lors du franchissement de la paroi sinusale
splénique, les corps figurés intraérythrocytaires non
déformables peuvent être expulsés du globule rouge
sans que ce dernier soit lysé. Ce processus original,
nommé épépinage (ou “pitting”), est mis en œuvre
physiologiquement pour éliminer du globule rouge
les résidus nucléaires. L’importance de ce phénomène
est abordée dans l'article consacré à l’utilisation de
l’artésunate i.v. en France.
Conclusion
La physiopathologie du paludisme implique donc
des mécanismes cellulaires, humoraux et immunolo-
giques qui s’avèrent complexes et intriqués. L’acteur
principal qui fait la spécificité de cette infection est
bien l’hématie parasitée qui interagit avec les cellules
de l’hôte. La rate est concernée par ces mécanismes
tout en exerçant un rôle de filtration et de régulation
cinétique. Tous ces mécanismes sont potentielle-
ment influencés par des polymorphismes de l’hôte et
du parasite, rappelant l’importance particulière de la
génétique dans l’expression de cette infection. Enfin,
ces mécanismes sont autant de pistes pour imaginer,
élaborer, voire évaluer de potentiels traitements
adjuvants (molécules diminuant la cytoadhérence,
immunomodulateurs, neuroprotecteurs, etc.). ■
1. Craig A, Scherf A. Molecules on the surface of the Plas-
modium falciparum infected erythrocyte and their role in
malaria pathogenesis and immune evasion. Mol Biochem
Parasitol 2001;115:129-43.
2. Crandall I, Sherman IW. Plasmodium falciparum (human
malaria)-induced modifications in human erythrocyte band
3 protein. Parasitology 1991;102:335-40.
3. Dondorp AM, Kager PA, Vreeken J, White NJ. Abnormal
blood flow and red blood cell deformability in severe
malaria. Parasitol Today 2000;16:228-32.
4. Dondorp AM, Desakorn V, Pongtavornpinyo W et al. Esti-
mation of the total parasite biomass in acute falciparum
malaria from plasma PfHRP2. PloS Med 2005;2:e204.
5. Schofield L, Hackett F. Signal transduction in host cells by
a glycosylphosphatidylinositol toxin of malaria parasites. J
Exp Med 1993;177:145-53.
6. Idro R, Jenkins NE, Newton CR. Pathogenesis, clinical
faetures and neurological outcome of cerebral malaria.
Lancet Neurol 2005;4:827-40.
7. Scuderi P, Sterling KE, Lam KS et al. Raised serum levels
of tumour necrosis factor in parasitic infections. Lancet
1986;2:1364-5.
8. Polder TW, Eling WM, Jerusalem CR, Wijers-Rouw M. A
cytochemical study of cerebrovascular lesions in mice infected
with Plasmodium berghei. J Neurol Sci 1991;101:24-34.
9. Orago AS, Facer CA. Cytotoxicity of human natural killer
(NK) cell subsets for Plasmodium falciparum erythrocytic
schizonts: stimulation by cytokines and inhibition by
neomycin. Clin Exp Immunol 1991;86:22-9.
10. Schofield L, Grau GE. Immunological processes in malaria
pathogenesis. Nat Rev Immunol 2005;5:722-35.
11. Barry OP, Pratico D, Savani RC, FitzGerald GA. Modula-
tion of monocyte-endothelial cell interactions by platelet
microparticles. J Clin Invest 1998;102:136-44.
12. Grau GE, Mackenzie CD, Carr RA. Platelet accumulation
in brain microvessels in fatal pediatric cerebral malaria. J
Infect Dis 2003;187:461-6.
13. Combes V, Taylor TE, Juhan-Vague I et al. Circulating
endothelial microparticles in Malawian children with
severe falciparum malaria complicated with coma. JAMA
2004;291:2542-4.
14. Faille D, Combes V, Mitchell AJ et al. Platelet micro-
particles: a new player in malaria parasite cytoadhe-
rence to human brain endothelium. FASEB J 2009;23:
3449-58.
15. Combes V, Coltel N, Alibert M et al. ABCA1 gene deletion
protects against cerebral malaria: potential pathogenic
role of microparticles in neuropathology. Am J Pathol
2005;166:295-302.
16. Pankoui Mfonkeu JB, Gouado I, Fotso Kuaté H. Elevated
cell-specific microparticles are a biological marker for
cerebral dysfunctions in human severe malaria. PLoS One
2010;5:e13415.
17. Snow RW, Marsh K. New insights into the epidemio-
logy of malaria relevant for disease control. Br Med Bull
1998;54:293-309.
18. Imbert P, Rapp C, Buffet PA. Pathological rupture of the
spleen in malaria: analysis of 55 cases (1958-2008). Travel
Med Infect Dis 2009;7:147-59.
19. Buffet PA, Safeukui I, Deplaine G et al. The pathogenesis
of Plasmodium falciparum malaria in humans: insights from
splenic physiology. Blood 2011;117:381-92.
20. Scherf A, Pouvelle B, Buffet PA, Gysin J. Molecular
mechanisms of Plasmodium falciparum placental adhesion.
Cell Microbiol 2001;3:125-31.
21. Groom AC, Schmidt EE, MacDonald IC. Microcircula-
tory pathways and blood flow in spleen: new insights from
washout kinetics, corrosion casts, and quantitative intra-
vital videomicroscopy. Scanning Microsc 1991;5:159-73;
discussion 173-4.
22. Ho M, White NJ, Looareesuwan S et al. Splenic Fc
receptor function in host defense and anemia in acute
Plasmodium falciparum malaria. J Infect Dis 1990;161:
555-61.
23. Looareesuwan S, Ho M, Wattanagoon Y et al. Dynamic
alteration in splenic function during acute falciparum
malaria. N Engl J Med 1987;317:675-9.
24. Safeukui I, Buffet PA, Deplaine G et al. Quantita-
tive assessment of sensing and sequestration of sphe-
rocytic erythrocytes by human spleen. Blood 2012;120:
424-30.
25. Buffet PA, Milon G, Brousse V et al. Ex vivo perfusion of
human spleens maintains clearing and processing functions.
Blood 2006;107:3745-52.
26. Deplaine G, Safeukui I, Jeddi F et al. The sensing of poorly
deformable red blood cells by the human spleen can be
mimicked in vitro. Blood 2011;117:e88-95.
27. Safeukui I, Correas JM, Brousse V et al. Retention of
Plasmodium falciparum ring-infected erythrocytes in the
slow, open microcirculation of the human spleen. Blood
2008;112:2520-8.
28. Tiburcio M, Niang M, Deplaine G et al. A switch in
infected erythrocyte deformability at the maturation and
blood circulation of Plasmodium falciparum transmission
stages. Blood 2012;119:e172-80.
29. Buffet PA, Safeukui I, Milon G, Mercereau-Puijalon
O, David PH. Retention of erythrocytes in the spleen: a
double-edged process in human malaria. Curr Opin Hematol
2009;16:157-64.
30. Keenihan SH, Gramzinksi R, Ratiwayanto S et al. Plas-
modium falciparum. Mechanisms of innate and acquired
protection against Plasmodium falciparum in Javanese
transmigrant adults and children newly resident in malaria-
endemic Northwest Papua. Adv Exp Med Biol 2003;531:
83-102.
31. Sanyal S, Egée S, Bouyer G et al. Plasmodium falciparum
stevor proteins impact erythrocyte mechanical properties.
Blood 2012;119:e1-8.
32. Chotivanich K, Udomsangpetch R, McGready R et al.
Central role of the spleen in malaria parasite clearance.
J Infect Dis 2002;185:1538-41.
Références bibliographiques
1
/
5
100%