none -défini

Particularités des cancers
du sujet agé
Au 1er janvier 2010, le Centre René Huguenin
devient l’Hôpital RenéHuguenin,
un établissement de soins, d’enseignement
et de recherche de l’Institut Curie
HÔPITAL RENÉ HUGUENIN
Docteur Etienne Brain
Oncologie Médicale

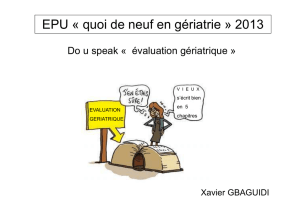
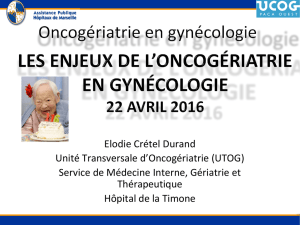
Projected number of cancer cases for 2000–2050 by age group (<45, 45–64, 65–84, 85+) based
on projected census population estimates and delay-adjusted SEER-17 cancer incidence
rates.
Hayat M J et al. The Oncologist 2007;12:20-37
©2007 by AlphaMed Press
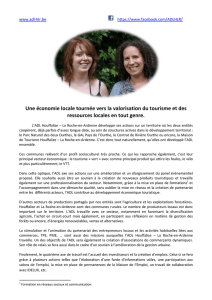
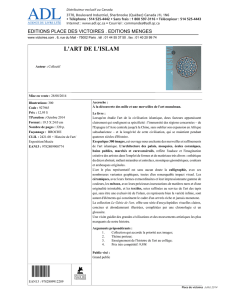
Incidence du cancer de 2010 à 2030 (Smith JCO 2009)
•+11% < 65A
•+67% > 65A

Les plus fréquents chez le sujet âgé
Cancer Statistics in the USA 2008, CA Cancer J Clin 2008

Pourquoi cette question ?
1. Les sujets âgés peuvent bénéficier des
traitements
2. Le nihilisme thérapeutique : les sujets âgés ne
reçoivent pas de traitement
3. L’enthousiasme thérapeutique aveugle : les
sujets âgés reçoivent un traitement « futile »
4. Places du gériatre et de l’oncologue

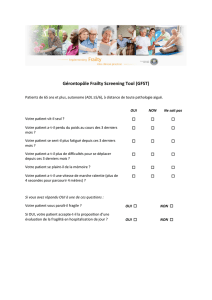
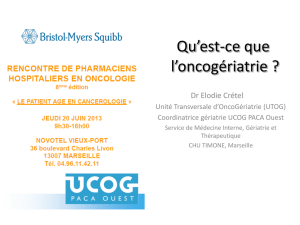
Definition of “old” x ageing heterogeneity
Age Top 25th%
Fit 50th%
Intermediate Lowest 25th%
Sick
50 36 28.5 19.6
70 18 12.4 6.7
75 14.2 9.3 4.9
80 10.8 6.7 3.3
85 7.9 4.7 2.2
90 5.8 3.2 1.5
95 4.3 2.3 1
Men life expectancy
Walter. JAMA 2001
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
1
/
38
100%