Cancers du nourrisson : 6tude 6pid6m

Cancers du nourrisson
:
6tude 6pid6m
L.
Hessissen,
A.
Kili,
M.
El Khorassani, N. Othmani,
M.N.
Nachef,
M.
Khattab,
F.
Msefer Alaoui
-
Unit& d3Hdmato-Oncologie Pddiatrique, Hdpital d'Enfants, Rabat
RCsumC
Le cancer du jeune nourrisson est rare. La diffkrence dans la distribution des types de cancer dans cette tranche d'bge fait
que 1a presentation clinique et I'approche therapeutique different de celles des autres tranches d'bge. Cette etude est une
analyse r6trospective de tous les cas de cancer diagnostiquts au sein de ['Unite d'H6matologie et d'oncologie PBdiatrique
de Rabat chez des nourrissons lgts de moins d'un an. Nous avons analysd l'tpidemiologie, la repartition des diffkrents
types de cancer et 1'Cvolution sous traitement. Sur une pCriode de 11 ans, allant de Janvier 1992
a
dCcembre 2002,90 enfants
d'lge infirieur
a
un an ont ett suivis pour une pathologie tumorale. Le neuroblastome a Ctt retrouvtt chez 31 patients et
constitue la tumeur la plus frCquente (34%), le nCphroblastome 'vient en deuxieme position (IS%), les leucemies aigu&s
13%,
les tumeurs m6senchymateuses 11% et le rttinoblastome 8%. Les tumeurs germinales ont ete retrouvees dans
6
cas
et l'htpatoblastome dans 3 cas. Le traitement a consist6 en une chimiothkrapie dans 73 cas. La chirurgie a etC le seul trai-
tement dans 7 cas.
La
radiotherapie a Cte utilisee dans
5
cas. La survie sans Cvknement
a
130 mois a kt6 de 47.2%
i
9% et
la survie globale a CtC de 66.8%
'1
7%. La distribution du cancer chez le jeune nourrisson est differente de cellc que l'on
retrouve chez I'enfant plus LgC. L'approche diagnostique et thttrapeutique doit tenir compte de ces particularites.
Mots
clCs
:
Cancer. ChimiothCrapie. Nourrisson.
Summary
The cancer of infant is a rare event. The differences of infant cancer types lead to a different approach of diagnosis and
treatment. This study is a retrospective analysis of all cases of cancer in infants less than 1 year-old in the Paediatric
Oncology Unit of Rabat Children Hospital. From January 1992 to December 2002, 90 infants were followed-up for cancer.
Neuroblastoma was the most frequent tumour (34%), followed by nCphrob1astoma (lS%), leukaemia (l3%), sarcoma (1 1%)
and retinoblastoma (8%). Germinal cell tumours were found in 6 cases and hepatoblastoma in
3
cases. Treatment consisted
in chemotherapy in 73 cases. Surgery alone was done in 7 cases and radiotherapy in
5.
The event free survival rate at 130
months was 47.2%
9%
and the overall survival 66.8%
*
7%. In conclusion, the distribution of cancer in the young infant
is different of the older child. The diagnostic and therapeutic approach must take these characteristics into account.
Key
words
:
Cancer. Chemotherapy. Infant.
Introduction
Le cancer du jeune nourrisson est rare
[I],
le neuro-
blastome etant la tumeur la plus frdquente chez le nour-
risson de moins d'un an. La diffdrence dans la distri-
bution des types de cancer dans cette tranche d'lge fait
que
la
prdsentation clinique et l'approche therapeutique
different de celles des autres tranches d'gge
[2,3,4].
La
prise en charge du cancer du nourrisson doit Cgalement
tenir compte des particularites liees
a
I'lge notamrnent
l'imaturitd et la croissance. L'apparition d'un cancer
dans cette tranche d'lge efface la distinction qui existe
entre I'embryogenbe, la tdratogenbse et la carcinoge-
nese
[5].
Chez le nourrisson, le processus d'oncogenese
est Ctroitement lie
a
celui de la teratogenese
[6].
Cette etude est une analyse r4trospective
de
tous
les cas
de
cancers diagnostiques au sein de 1'UnitC

Rzv
Mar
%la1
Enf
2005,
7
16-20
17
dlHematologie et d'oncologie Pediatrique de l'H6pital
d7Enfants de Rabat chez des nourrissons Bges de moins
d'un an. Nous avons analyse la ripartition des diffirents
types de cancer, les moyens diagnostiques et l'approche
thkapeutique.
Patients et MCthode
Cette etude inclut tous les patients d'iige strictement
superieur
a
1
mois et inferieur
B
12 mois, suivis pour un
cancer au sein de 1'UnitC d7Hematologie et dYOncologie
PCdiatrique de Rabat. La periode de l'itude s'est etalee
de janvier 1992
a
decembre 2002. Le diagnostic de can-
cer a ete etabli grbce aux donnies de l'imagerie etiou des
marqueurs biologiques evou de la
cyto-histologic.
Les
marqueurs biologiques utilises etaient I'a-fceto-proteine
et les PHCG sanguins et les catCcholamines urinaires
(VMA,
HVA
et dopamine).
L'analyse a concerne l'bge au diagnostic, le sexe et
les antecedents du patient en particulier la consangui-
nite, les malformations et le cancer familial. Nous avons
Cgalement etudie la distribution par type de cancer, le
moyen utilise pour poser le diagnostic, le traitement
utilise ainsi que l'evolution du malade. Ont it6 con-
sideres comme Cvenements le decks, la rechute et la
rksistance. La sunlie a
PtC
calculee par !a mCthode de
Xaplan Meier.
Sur une periode de I1 ans, 90 cas de cancers chez
le nourrisson de moins d'un an ont Cte recenses, cons-
tituant ainsi environ
3,4%
des cas de cancer de l'enfant
rraites dans l'unite durant cette periode. L'bge midian au
diagnostic Ctait de 6,5 mois. Le sex ratio mile/femelle
Gtait de
1,4.
Nous avons retrouve des anteddents de
cancer dans les familks de 5 enfants (5,5%), dont 2 cas
de cancer dans la fratrie. Le frere d'un nourrisson atteint
d'un rhabdomyosarcome (RILIS) avait ete suivi pour un
neuroblastome (NB), un autre nourrisson presentait une
fome familiale de retinoblastome
(RBI.
Les parents
Gtaient consanguins dans 10% des cas.
La repartition selon le type de cancer est rapportee
dans le tableau
1.
Le neuroblastome a constitlid la tumeur
!a
plus frequente, avec
34,5O/0
des cas, suivi par ie nCph-
roblastome (15,5%) et la leuckmie
(1
1%). Les tumeurs
du systeme nerveux central ont constitue 1% des cas
de cancer. Sur les 31 cas de neuroblastome, la mediane
d'iige etait de
4
mois avec des extrzmes allant de
40
jours
a
10 mois. Le diagnostic a Cte etabli sur les donnies de
l'imagerie dans 13 cas, l'etude histologique dans 6 cas
et cytologique dans 5 cas;
4
cas ont ete diagnostiques sur
les donnees de l'imagerie et les resultats des marqueurs
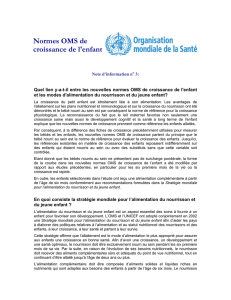
et un cas sur I'histologie et les marqueurs. Le neuroblas-
tome s'est presente sous forme d'un syndrome de Pepper
dans 13 cas (Fig.
1)
:
l'bge median etait de
4
mois avec
des extremes allant de 40 jours
a
9
mois. Dans les autres
cas, la localisation etait abdominale chez
8
nourrissons,
thoracique chez
4
nounrissons, et mediastinale chez
3
nourrissons. Trois nourrissons ont presente un syndrome
de Hutchinson avec une localisation surrinalienne dans 2
cas et un cas de neuroblastome abdominal median.
Tableau
I.
Repartition des differents types de cancer.
Nombre
de
cas
96
Neuroblastome
Nephroblastoine
Leucemie
Sarcome
Tutneurs gemlnales
RCttnoblastome
Hipatoblastome
Tumeur
SNC
Lymphome non Hodgkinien
Autres
SNC
sybteme nerveuu central
Fig.1.
TDM abdominale
:
hdpatomkgalie nodulaire typique
d'un syndrome de Pepper.

18
Rev
Mar
Ma1
Enf
2005.7
.
16-20
Dans les
14
cas de nephroblastome, le diagnostic vie sans CvCnement chez 1es nourrissons leuc6miques
a kte base initialement sur l'aspect echographique, et 6tait de 16,7%.
confirme en post-optratoire sur 1'6tude histologique de
la piece de nkphrectomie.
Le diagnostic des
8
cas de tumeurs germinales a ete
histologique dans 7 cas (trois cas diagnostiques par his-
tologie et marqueurs) et sur les donnees de l'imagerie
dans 1 cas. La localisation Ctait sacro-coccygienne dans
2 cas et pelvienne dans 2 autres cas. Les 4 autres locali-
sations etaient
:
le poumon, la parotide, l'abdomen et le
cou. Sur le plan histologique,
il
s'agissait d'un ttratome
dans
7
cas et d'un choriocarcinome dans
1
cas.
Suwie sans evenements
Douze cas de leuctmie ont ete diagnostiques dont 5
etaient des leuckmies aigues lymphoblastiques (LAL),
6 des leuckmies aigues mytloblastiques (LAM) et enfin
un cas de leuctmie myelomonocytaire chronique.
Le diagnostic des
7
cas de
RB
a CtC retenu sur l'aspect
histologique de la piece d'dnucleation. L'hkpatoblastome
a Ctk diagnostiquk dans les 3 cas sur
un
aspect evocateur
a
l'imagerie et des marqueurs positifs (a-fceto-prothe).
=
5'
Les tumeurs sarcomateuses ont reprksente
1
1% des
F
4
'
cas (10 cas). Le rhabdomyosarcome (RMS) a ete retrou-
3
1
vC dans 6 cas, celui-ci etait localis6 dans l'orbite dans
2
2
1
cas, le pied dans 1 cas et le testicule dans
1
cas. Les tu-
1
meurs sarcomateuses non RMS etaient representees par
Le traitement a consisti en une chimiotherapie dans
73 cas. Dans 21 cas la chimiotherapie, a tte associCe
a
une chirurgie. La chirurgie a ete le seul traitement
dans 7 cas. La radiothkrapie a CtC utilisCe dans 5 cas
(1
cas de
RMS,
2
cas de nkphroblastome et 2 cas de
RB).
Dans 3 cas de syndrome de Pepper l'abstention thera-
peutique a Ct4 pr6conisCe. Sept patients sont decCdCs
ou ont Ctk perdus de we avant traitement. Sur les 90
patients suivis, 27 sont en remission complMe conti-
nue. Un CvCnement est survenu chez 25 patients
:
cinq
cas de rechute, 17 deces et
3
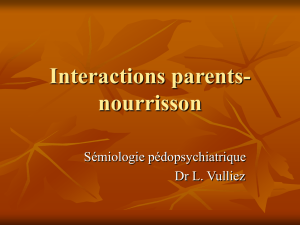
cas de resistance. Trente
huit patients ont ete perdus de vue. La survie sans kvk-
nement
a
130 mois a ete de 47,2%
i
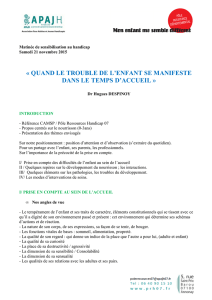
9% (Fig.2) et la
survie globale a CtC de 66,8%
=k
7% (Fig.3). L'anaIyse
de la survie selon le type de cancer est detaillte dans
le tableau
11.
Sur
les
17
patients dCctdCs,
5
etaient des
leucernies,
4
des
NB
et
3
des nephroblastomes. La sur-
0
Fig.2.
Courbe de survie sans evenements (SSE) des 90 cas de
cancer du nourrisson. SSE
a
130 mois
=
47,2%
9%.
0
*
l'angiosarcome dans
1
cas, le liposarcome dans
1
cas et
o
20 40 60 80
loo
120 140
le synovialosarcome dans 2 cas.
MOIS
Courbe de suwie globale
1.0
p
-
-
0
20 40 60 80 100 120 140
Mois
Fig.3.
Courbe de swie globale des 90 cas de cancer du
nourrisson. Survie globale
a
130 mois
=
66,8%
*
7%.
Tableau
11.
Survie sans Cvknements selon le type de cancer.
cpe
de cancer ~Vornbre de
Dkc2s
SSE
cas
&4
Neuroblastome 3
1
4
67
Nephroblastome 14
3
633
LeucCmies 12
5
16,:
Sarcomes 10 0 50
Tumeurs germinales
8
2 72,9
RCtinoblastorne
7
7
37.5
Autres
8
I
66.7

i;cv
M:tr
Ma1
Enf
2005;
7
:
16-20
19
Discussion
L'incidence du cancer chez I'enfant de moins d'un an
'1
ete esti~nke aux
USA
par le Xational Cancer Institute's
I
NCI)
a
2 18,4 cas pour un million d'enfants [l]. L'etio-
iogie du cancer chez le nouveau-ne et le nounisson
cst inconnue. Toutefois, des facteurs genetiques, intra-
uterins et environnementaux ont Cte incrimines. Des
formes genetiques hereditaires ont ete decrites pour le
nephroblastome. le RB, l'hepatoblastome et la leucemie
[6]. Ces formes ont tendance
a
se developper chez le
jeune nourrisson, contrairement aux formes sporadiques
qui se developpent chez I'enfant plus ige [7,8]. La trans-
mission transplacentaire de cancers tels que la leucemie
ou le melanome a Cte decrite depuis longtemps, mais elle
reste cependant exceptionnelle [9]. Dans notre drie, la
consanguinite a ete retrouvee dans 10% des cas, ce qui
est inferieur au taux de consang~~inite dans la population
marocaine. Les cas familiaux ont Cte decrits chez 5,594
de nos patients et aucun cas de syndrome predisposant
au cancer n'a ete deerit, mais notre enquCte est retros-
pective et certaines donnees ont ete probablement ma1
recueillies.
Les donnees du NCI ont montre une augmentation
de I'incidence annuelle du cancer du nourrisson qui est
passee de 183,4/milhon en 1970
a
189 en 1980 et 220 en
1990. Cette augmentation peut gtre expliquke par I'uti-
lisation de plus en plus frequente d'examens ultrasono-
graphiques durant la grossesse et chez le nourrisson [I].
Les cancers les plus frequents dans cette tranche d'Bge
sont le NB, la leucemie, les tumeurs renales, les tumeurs
germinales, les sarcomes, le RB et les tumeurs du sys-
teme nerveux central (SXC) [2,10]. La distribution des
differents types de cancer selon les tranches d'5ge est
rapportee dans le tableau I11 [11,12]. Dans notre serie,
le NB est la tumeur la plus frequente alors que chez
I'enfant tigC de plus d'nn an la leucemie est le premier
cancer. La frequence des differents types de cancers du
nourrisson connait -des variations geographiques. Au
Japon, cette frequence est elevee probablement
a
cause
de la generalisation dl1 dCpistage du NB [13]. Contraire-
lnent
a
l'enfant plus Bgl, la leucemie, le nephroblastome
et le RB sont des cancers plus frequents chez Ies nour-
rissons de sexe feminin [lo]. En Sukde, la prevalence du
RB est Clevle 121.
La prise en charge therapeutique doit tenir compte
des particularitks likes
a
I'dge et qui peuvent Etre
Tableau
ill.
Distribution des differents types de cancer selon
l'2ge.
LeucCmie
Systeme nerveux
central
Neuroblastome
Lymphome
Rein
Sarcome
HCpatiqiie
Teratome
RCtinoblastome
Autres
a
l'origine d'une toxicite beaucoup plus importante.
Chez le nourrisson, la capacite de concentration du rein
est reduite, les enzymes gastro-intestinales sont imma-
tures et le SNC est incompletement myClinise [14]. La
demi-vie des drogues peut 2tre prolongee, et la toxicite
augmentee. L'ean corporelle constitue 80% du poids du
nourrisson et seulement 50% chez l'enfant plus Pge.
L'eau extracellulaire constitue environ 45% du poids
du corps
a
la naissance et 20%
a
un Bge plus tardif.
Cette particularit6 fait que i'utiiisation de la surface cu-
tanke n'est pas approprike pour le calcul des doses qui
doit se faire selon le poids en kilogrammes [15]. Tous
les protocoles de traitement utilises dans notre serie
precisent une reduction de
11'3
si le calcul des doses est
fait en utilisant Ia surface cutanee ou un ajustement des
doses en fonction du poids du corps. La chirurgie chez
le nourrisson doit tenir compte de la fragilite metaboli-
que et physiologique
[16].
Elle doit Ctre incluse dans un
plan de traitement pouvant associer une chimiotherapie
ou une radiotherapie qui alterent generalement le sys-
teme nutritionnel et immunitaire. La radiotherapie a un
r61e majeur dans le traitement de la plupart des tumeurs
de I'enfant, mais son utilisation chez le nounisson doit
se faire avec une trks grande prudence, car la severite
des effets secondaires est inversement proportionnelle
a
I'dge et aux doses [17]. Les donnees existantes mon-
trent une plus grande vulnerabilite du nourrisson
a
des
effets secondaires tels que les problemes de croissance,
I'alteration de la fonction de certains organes, en par-
ticulier le SNC, et
a
l'effet carcinogene de la radiothe-
rapie [17,15]. Dans notre sdrie la radiotherapie a it6
utilisie chez
5
patients.

20
Rev
Mar
Ma1
Enf
2005;
7
:
16-20
Le pronostic chez le nourrisson depend du type de
cancer
:
le NB et les tumeurs du rein sont de tres bon
pronostic, alors que la leucCmie et les tumeurs du SNC
sont agressives et de trks mauvais pronostic [19]. Parmi
nos
12
patients suivis pour leuctmie, un seul patient
Ctait en remission complkte au moment de l'ttude. Le
NB constitue environ li3 des tumeurs du nourrisson.
L'8ge au diagnostic et l'extension de la maladie sont
des facteurs pronostiques majeurs, mais ne sont pas les
seuls [20]. D'autres variables pronostiques ont kt6 identi-
fiCes, essentiellement l'amplification du proto-oncoghe
N-myc, la Non Specific Enolase et la ferritine [21]. Nous
n'avons utilise que 1'Bge et l'extension de la maladie
come facteurs pronostiques pour nos cas de NB. Le
syndrome de Pepper est une fonne particulikre de
NB
qui
peut rdgresser spontantment dans 80% des cas [22,23].
Dans notre sene, 3 patients suivis pour un syndrome de
Pepper sont en remission complbte continue sans aucun
traitement.
Certaines recommandations ont Cte emises pour la prise
en charge des cancers du nourrisson [19]: Cviter l'image-
rie complexe non contributive; utiliser les examens echo-
graphiques en premier; faire les dosages des VMA/HVA
urinaires, afmto-protkines et autres marqueurs appropries
A
chaque type de tumeur; utiliser le mtdullogramme aussi
souvent que possible; Cviter la chirurgie mutilante; utiliser
la chimiothkapie quand elle est clairement indiquke, en
calculant selon le poids du corps et en faisant attention
a
la toxicite; eviter la radiothkrapie; Cvaluer frequemment la
rdponse au traitement; faire un conseil gtndtique.
En conclusion.
le cancer du nourrisson necessite une
demarche diagnostique simple et la moins traumatisante
possible. Le traitement doit &re adapt6 aux particularitks
likes
B
1'8ge et le conseil gendtique doit faire partie de la
prise en charge.
1.
Gurney
JG,
Ross JA, Wall DA, Bleyer WA and al. Infant cancer
in the US: Histology-specific incidence and trends, 1973 to 1992.
J Pediatr Hematol Oncol. 1997, 19: 428-32.
2. Birch
JM,
Blair
V,
The epidemiology of infant cancers. Br J
Cancer. 1992,66: S2- S4.
3. Bader JL, Miller RW.US cancer incidence and mortality in the
first year of life. Am
J
Dis Child. 1979* 133: 157-9.
4. Bleyer WA. The past and future of cancer
in
the young. Pediatr
Dent. 1995, 17: 285-90.
5. Bolande
RP.
Neoplasia of early life and
its
relationship to
teratogenesis. Perspect Pediatr Pathol. 1976,3: 145-51.
6. Kenney LB, Reaman GH. Special considerations for the
infant with cancer. In: Principle2 and practice of pediatric
oncology. Philip A Pizzo, David G Poplack, Editors. 3rd edition.
Philadelphia. Lippincott-Raven Publishers. 1997.
p
343-73.
7. Knudson AG, Strong
LC.
Mutation and cancer: a model for
Wilms' tumor of the kidney. JNat Cancer Inst. 1972,48:313.
8. Reynolds T. Causes of childhood leukemia beginning to emerge.
J Nat Cancer Inst. 1998,90: 8-10.
9. Li FP, Fraumeni
JF
Jr.
Soft tissue sarcomas, breast cancer and
other neoplasms: a familial syndrome? Ann Int Med. 1969, 71:
747-52.
10. Gurney JG, Severson
RK,
Davis S, Robinson LL. Incidence of
cancer in children in the United States. Cancer. 1995,75: 2186-95.
11. Bader JL, Miller RW. U.S. cancer incidence and mortality in the
first year of life. Am J Dis Child. 1979, 133: 157.
12. Hanson MR, Mulvihill JH. Epidemiology of cancer in the young.
In: Cancer in the young. Levine AS, ed. New York. Masson
Publishing. 1982. p3.
13. Bessho F. Is there a future for neuroblastoma mass screening?
Med Pediatr Oncol. 1998,3 1:106-10.
14. Morgan E, Baum EI Breslow
N,
Takashima J, D'Angio
G.
Chemotherapy-related toxicity in infants treated according to the
Second National
Wilms'
Tumor Study.
J
Clk Oncol. 1988.6: 5 1-5.
15. Friis-Hansen B. Body water compartments
in
children: changes
during growth and related changes in body composition.
Pediatrics. 1961.28: 169-81.
16. De Lorimier AA, Harrison
MR.
Surgical treatment of tumors in
the newborn. Am J Pediatr Hematol Oncol. 1983,3: 271.
17. Litttnan
P,
D'Angio GJ. Radiation therapy in the neonate. Am
J
Pediatr Hematol Oncol. 198 1, 3: 279
18. Meister LA, Meadows AT. Late effects of childhood cancer
therapy. Curr Probl Pediatr. 1993.23: 102-3 1.
19. Vasilatou-Kosmidis H. Cancer in infants. Med Pediatr Oncol.
2003,41: 7-9.
20. Isaacs H. Congenital and neonatal malignant tumors: a 28-year
experience. Am J Pediatr Hematol Oncol. 1987.9: 121.
21. Look AT, Hayes FA, Shuster JJ. Clinical relevance of tumor cell
ploidy and N-myc amplification in childhood neuroblastoma. J
Clin Oncol. 199
1,9: 58 1.
22. Strother D, Shuster
JJ,
McWilliams N, Nitschke R, Smith EI,
Joshi VJ and al. Results of pediatric oncology group protocol
8104 for infants with stages D and DS neuroblastoma. J Pediatr
Hematol Oncol. 1995, 17: 254-9.
23. Nitschke R, Humphrey GB, Sexauer CL, Smith El.
Neuroblastoma: therapy for infants with good prognosis. Mcd
Pediatr Oncol. 1983, 11: 154-8.
1
/
5
100%