carcinome medullaire de la thyroide : prise en charge ultra

ANATOMIE
EXAMEN CLINIQUE

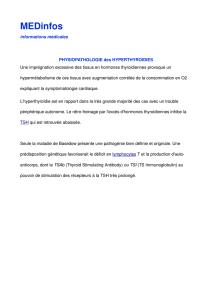
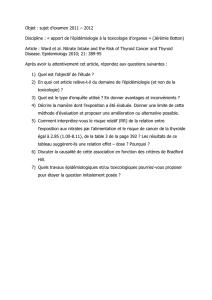
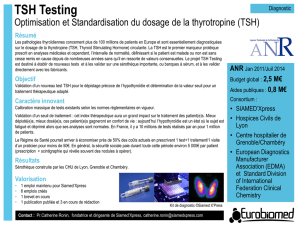
Figure 21-1. The normal
anatomy of the neck in the
region of the thyroid gland.
(With permission from Halsted
WS: The operative story of
goiter. Johns Hopkins Hosp
Rep 19:71, 1920).

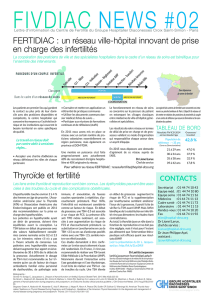
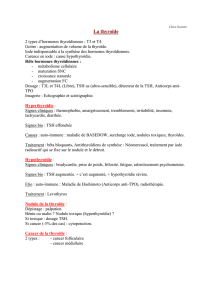
Figure 21-2. Large goiters are prevalent in areas of
iodine deficiency. (A). A woman from Switzerland
operated upon by Dr. Theodor Kocher (From Kocher T:
Zur pathologie und therapie deKropfes (parts I and 2).
Dtsch Z Chir 4, 1874 ) (B). One hundred years later, large
goiters still occur in many parts of the world, as
demonstrated in this woman from a mountainous region
of Viet Nam, 1970.
A
B

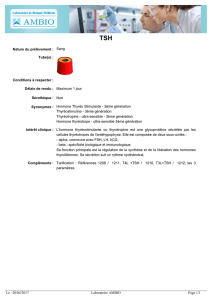
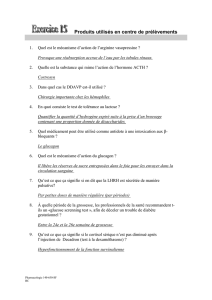
Figure 21-4. The location of 204 recurrent laryngeal nerves in dissection
of 102 cadavers. Note that the recurrent laryngeal nerve was found anterior
to the tracheoesophageal groove in 42 percent of cases and within the
thyroid gland in 3.9 percent of cases. In both of these locations, the nerve
is more prone to be damaged if its course is not carefully visualized by the
surgeon. (With permission from SkandalakisJE, Droulias C, Harlaftis N et
al: The recurrent laryngeal nerve. Am Surg 42:629, 1976).

 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
1
/
106
100%