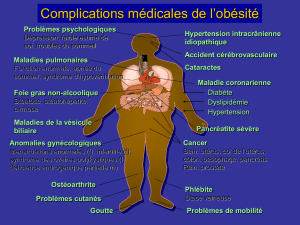
CHIRURGIE BARIATRIQUE : DÉPISTAGE DE L`HTP CHEZ LE SAOS

CHIRURGIE BARIATRIQUE :
DÉPISTAGE DE L’HTP CHEZ LE SAOS
DONAT Alexis Hôpital Antoine Béclère

Obésité et SAOS?

cardiovascular disease accelerates disease progression, and
whether treatment of sleep apnea results in clinical im-
provement, fewer cardiovascular events, and reduced
mortality.
Experimental approaches directed at addressing these issues
are limited by several considerations. First, the close association
between obesity and OSA often obscures differentiation be-
tween the effects of obesity, the effects of OSA, and the effects
of synergies between these conditions. Second, multiple comor-
bidities, including cardiovascular disease, metabolic syndrome,
and diabetes, often are present in patients with sleep apnea.
Hence, it becomes unclear whether abnormalities evident in the
sleep apnea patient with cardiovascular disease are secondary to
the sleep apnea, the cardiovascular condition, or both. The third
consideration relates to randomization of sleep apnea patients to
active or no treatment. Although this is a reasonable strategy for
identifying the mechanistic and prognostic consequences of
sleep apnea per se, it is limited by the difficulties inherent in any
placebo-controlled treatment study of sleep apnea and the need
to consider treatment in patients with severe daytime somno-
lence, even in the absence of associated cardiovascular disease.
Definitions, Classifications, Diagnosis,
and Pathophysiology
Obstructive Sleep Apnea
OSA is characterized by repetitive interruption of ventilation
during sleep caused by collapse of the pharyngeal airway. An
obstructive apnea is a !10-second pause in respiration
associated with ongoing ventilatory effort. Obstructive hy-
popneas are decreases in, but not complete cessation of,
ventilation, with an associated fall in oxygen saturation or
arousal. A diagnosis of OSA syndrome is accepted when a
patient has an apnea-hypopnea index (AHI; number of apneas
and hypopneas per hour of sleep) !5 and symptoms of
excessive daytime sleepiness
20
(Figure 1 and Table 1; see
Table 2
5
for definitions of terms).
Although hypopneas constitute the majority of disordered
breathing events, there is some controversy regarding the
optimal criteria for definition of hypopneas. A recent analysis
of data from !6000 adults participating in the Sleep Heart
Health Study noted that hypopneas accompanied by oxyhe-
moglobin desaturation of !4% were associated with preva-
lent cardiovascular disease independently of confounding
covariates.
21
In contrast, no association was observed be-
Figure 1. Partial and complete airway
obstruction resulting in hypopnea and
apnea, respectively. Reprinted from Hahn
PY, Somers VK. Sleep apnea and hyperten-
sion. In: Lip GYH, Hall JE, eds. Comprehen-
sive Hypertension. St. Louis, Mo: Mosby;
2007:201–207. Copyright Elsevier 2007.
Used with permission.
Table 1. Obstructive Sleep Apnea
Signs, symptoms, and risk factors
Disruptive snoring
Witnessed apnea or gasping
Obesity and/or enlarged neck size
Hypersomnolence (not common in children or in heart failure)
Other signs and symptoms include male gender, crowded-appearing
pharyngeal airway, increased blood pressure, morning headache, sexual
dysfunction, behavioral changes (especially in children)
Screening and diagnostic tests
Questionnaires
Holter monitoring
Overnight oximetry
Home-based/ambulatory unattended polysomnography
In-hospital attended overnight polysomnography
Treatment options
Positional therapy
Weight loss
Avoidance of alcohol and sedatives
Positive airway pressure
Oral appliances
Surgery
Uvulopalatopharyngoplasty
Tonsillectomy
Tracheostomy
Somers et al AHA/ACCF Sleep Apnea and Cardiovascular Disease 1081
by guest on December 18, 2015http://circ.ahajournals.org/Downloaded from
Syndrome d’apnée obstructive du sommeil
! Fréquent : 70 % des patients de chirurgie bariatrique
! Mécanisme : interruption répétitive de la ventilation
! durant le sommeil
! par collapsus pharyngé
cardiovascular disease accelerates disease progression, and
whether treatment of sleep apnea results in clinical im-
provement, fewer cardiovascular events, and reduced
mortality.
Experimental approaches directed at addressing these issues
are limited by several considerations. First, the close association
between obesity and OSA often obscures differentiation be-
tween the effects of obesity, the effects of OSA, and the effects
of synergies between these conditions. Second, multiple comor-
bidities, including cardiovascular disease, metabolic syndrome,
and diabetes, often are present in patients with sleep apnea.
Hence, it becomes unclear whether abnormalities evident in the
sleep apnea patient with cardiovascular disease are secondary to
the sleep apnea, the cardiovascular condition, or both. The third
consideration relates to randomization of sleep apnea patients to
active or no treatment. Although this is a reasonable strategy for
identifying the mechanistic and prognostic consequences of
sleep apnea per se, it is limited by the difficulties inherent in any
placebo-controlled treatment study of sleep apnea and the need
to consider treatment in patients with severe daytime somno-
lence, even in the absence of associated cardiovascular disease.
Definitions, Classifications, Diagnosis,
and Pathophysiology
Obstructive Sleep Apnea
OSA is characterized by repetitive interruption of ventilation
during sleep caused by collapse of the pharyngeal airway. An
obstructive apnea is a !10-second pause in respiration
associated with ongoing ventilatory effort. Obstructive hy-
popneas are decreases in, but not complete cessation of,
ventilation, with an associated fall in oxygen saturation or
arousal. A diagnosis of OSA syndrome is accepted when a
patient has an apnea-hypopnea index (AHI; number of apneas
and hypopneas per hour of sleep) !5 and symptoms of
excessive daytime sleepiness
20
(Figure 1 and Table 1; see
Table 2
5
for definitions of terms).
Although hypopneas constitute the majority of disordered
breathing events, there is some controversy regarding the
optimal criteria for definition of hypopneas. A recent analysis
of data from !6000 adults participating in the Sleep Heart
Health Study noted that hypopneas accompanied by oxyhe-
moglobin desaturation of !4% were associated with preva-
lent cardiovascular disease independently of confounding
covariates.
21
In contrast, no association was observed be-
Figure 1. Partial and complete airway
obstruction resulting in hypopnea and
apnea, respectively. Reprinted from Hahn
PY, Somers VK. Sleep apnea and hyperten-
sion. In: Lip GYH, Hall JE, eds. Comprehen-
sive Hypertension. St. Louis, Mo: Mosby;
2007:201–207. Copyright Elsevier 2007.
Used with permission.
Table 1. Obstructive Sleep Apnea
Signs, symptoms, and risk factors
Disruptive snoring
Witnessed apnea or gasping
Obesity and/or enlarged neck size
Hypersomnolence (not common in children or in heart failure)
Other signs and symptoms include male gender, crowded-appearing
pharyngeal airway, increased blood pressure, morning headache, sexual
dysfunction, behavioral changes (especially in children)
Screening and diagnostic tests
Questionnaires
Holter monitoring
Overnight oximetry
Home-based/ambulatory unattended polysomnography
In-hospital attended overnight polysomnography
Treatment options
Positional therapy
Weight loss
Avoidance of alcohol and sedatives
Positive airway pressure
Oral appliances
Surgery
Uvulopalatopharyngoplasty
Tonsillectomy
Tracheostomy
Somers et al AHA/ACCF Sleep Apnea and Cardiovascular Disease 1081
by guest on December 18, 2015http://circ.ahajournals.org/Downloaded from
Pas de ventilation pendant 10
secondes + efforts inspiratoires
Baisse du débit inspiratoire de 50%
+ désaturation
Recommandations pour la pratique clinique du syndrome d’apnées hypopnées obstructives du sommeil de l’adulte
Rev Mal Respir 2010
Peromaa-haavisto et al. Prevalence of Obstructive Sleep Apnoea Among Patients Admitted for Bariatric Surgery. A
Prospective Multicentre Trial. Obes Surg 2015.

Syndrome d’apnée obstructive du sommeil
Recommandations pour la pratique clinique du syndrome d’apnées hypopnées obstructives du sommeil de l’adulte
Rev Mal Respir 2010
Peromaa-haavisto et al. Prevalence of Obstructive Sleep Apnoea Among Patients Admitted for Bariatric Surgery. A
Prospective Multicentre Trial. Obes Surg 2015.
! Diagnostic :
! Somnolence diurne
! Ronflements, sensation d’étouffement nocturne, nycturie
! Index apnées + hypopnées / h > 5
! Sévère si index apnées + hypopnées / h > 30
! Fréquent : 70 % des patients de chirurgie bariatrique
! Mécanisme : interruption répétitive de la ventilation
! durant le sommeil
! par collapsus pharyngé

Définition
Physiopathologie
La littérature médicale
Hypertension pulmonaire et SAOS ?
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
1
/
40
100%