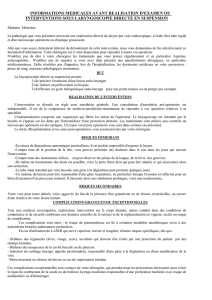
Cancers Pharyngo Laryngés

Cancers Pharyngo-Laryngés:
- cancers du larynx
- cancers de l’hypopharynx
Candice Carola
Interne onco hémato 7ème semestre
CHU Amiens
Tuteur : Pr Page Cyril

Généralités
•Epidémiologie : alcool + tabac
•K pidermodes oropharynx / hypopharynx / larynx / cavité orale
en France plus de 90 % des cancers des VADS.
•Anatomopathologie : carcinome épidermoïde
•Diagnostic souvent tardif (conditions socio-culturelles)
•Extension locale et lymphonodale
•Traitement : chirurgie et/ou RT et/ou CT
•Risques évolutifs : récidives locale / lymphonodale / M+ / 2ème K
HAS / Service Maladies chroniques et dispositifs d’accompagnement des malades / INCa / Dpartement des recommandations professionnelles Novembre 2009

Rappels anatomiques

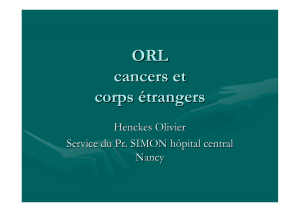
Larynx (1)

Larynx (2)
Etage supra-glottique:
- Margelle
- Vestibule
- Plis vestibulaires
- Ventricule
Etage glottique:
- Pli vocal
Etage infra-glottique:
- Concavité Cricoïde
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
1
/
32
100%