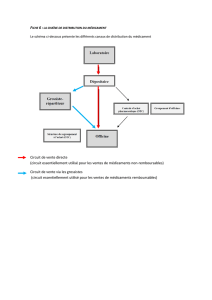
Registre des médicaments - Innovative Medicines Canada

Registre des médicaments
PRÉSENTÉ PAR :
linformationestlameilleureprescription.org

Renseignementspersonnels
Nom :____________________________________
Datedenaissance:____________________________________
Numérodetéléphone:_________________________________
Numérod’assurancemaladie:________________________________
Assurancesantéprivée:
Nom :_______________________________________
Numérodetéléphone:________________________________
Numérodecontrat/police:_________________________________
Personneàrejoindreencasd’urgence:
Nom :_______________________________________
Lienaveclapersonneàrejoindre:___________________________
Numérodetéléphone:________________________________
Groupesanguin :________________________________
Allergies:
Médecindefamille:
Nom:________________________________________
Numérodetéléphone:____________________________________
Numérodetélécopieur:____________________________________
Pharmaciecommunautaire:
Nom:________________________________________
Numérodetéléphone:_________________________________
Type:Allergiqueà:Réaction:
Médicament
Alimentaire
Environnemental
Veuillezconservervosrenseignementsdansunendroitsécuritaireetvousrappelerquelescommunicationsélectroniques,incluantle
courriel,peuventnepasêtresécuritaires.

Calendrierdesmédicaments
Nom:____________________________
Dernièremiseàjour:_______________
Quelmédicament
dois‐jeprendre?
Pourquoidois‐je
prendrece
médicament?
Àquoiressemblele
médicament?
Quandetcommentdois‐
jeprendrece
médicament?
Quiaprescritce
médicament?Notes
Matin
(petitdéjeuner)
Midi
(dîner)
Soir
(souper)
Aucoucher
Veuillezconservervosrenseignementsdansunendroitsécuritaireetvousrappelerquelescommunicationsélectroniques,incluantle
courriel,peuventnepasêtresécuritaires.

Carnetd’immunisation
Nom:_____________________
Vaccinépour:
Nomde
commercedu
vaccin
Date
d’administrationDoseSiteVoie
d’administration
Administrépar
(Nomettitredela
personnequi
administrelevaccin)
FabricantNumérode
lot
DT(diphtérieet
tétanos)
HépatiteA
HépatiteB
VPH(viruspapillome
humain)
Influenza
Méningiteà
méningocoques
ROR(rougeole,
oreillonsetrubéole)
Pneumocoque
DPT(diphtérie,
coquelucheet
tétanos)
Varicelle
Autre
Veuillezconservervosrenseignementsdansunendroitsécuritaireetvousrappelerquelescommunicationsélectroniques,incluantle
courriel,peuventnepasêtresécuritaires.

Listedesmédicaments
Nom:_____________________________
Dernièremiseàjour:________________
Quelmédicament
dois‐jeprendre?
Pourquoidois‐je
prendrece
médicament?
Àquoiressemblele
médicament?
Quandetcomment
dois‐jeprendrece
médicament?
Quiaprescritce
médicament?
Quandest‐cequej’ai
commencéàprendre
cemédicament?
Notes
Veuillezconservervosrenseignementsdansunendroitsécuritaireetvousrappelerquelescommunicationsélectroniques,incluantle
courriel,peuventnepasêtresécuritaires.
 6
7
8
9
10
11
6
7
8
9
10
11
1
/
11
100%