Mise à jour 2013 des lignes directrices du CANMAT sur la prise en

Mise à jour 2013 des lignes directrices du
CANMAT sur la prise en charge des patients
atteints d’un trouble bipolaire
Par : Sagar V. Parikh, M.D., FRCPC, et Benjamin Goldstein, M.D., Ph.D., FRCPC Membres exécutifs du Conseil
consultatif du CANMAT
Sagar V. Parikh, M.D., FRCPC
Président chargé de l’éducation, Toronto
Rédacteur, Troubles de l’humeur et de
l’anxiété – Conférences scientifiques
sagar[email protected]
Raymond W. Lam, M.D., FRCPC
Président exécutif, Vancouver
Sidney H. Kennedy, M.D., FRCPC
Président du groupe chargé de la dépression,
Toronto
Lakshmi N. Yatham, MBBS, FRCPC, MRCPsych
(R.-U.) – Président chargé des troubles
bipolaires, Vancouver
Jitender Sareen, M.D., FRCPC
Président du groupe chargé de l’anxiété,
Winnipeg
Roger S. McIntyre, M.D., FRCPC
Président – Développement commercial
et de la recherche, Toronto
Roumen Milev, M.D. Ph.D., FRCPsych, FRCPC
Président – Conférences internationales,
Kingston
Membres du Conseil
d’administration du CANMAT
Serge Beaulieu, M.D., Ph.D., FRCPC
Montréal
Glenda MacQueen, M.D. Ph.D., FRCPC
Calgary
Diane McIntosh, M.D., FRCPC
Vancouver
Arun V. Ravindran, M.B., Ph.D., FRCPC
Toronto
Association Canadienne pour le Traitement
des Troubles Anxieux et de l’Humeur
Bureau de l’éducation
Salle 9M-329, Toronto Western Hospital
399, rue Bathurst (Toronto) Ontario
CANADA M5T 2S8
Le CANMAT – ou Association Canadienne pour le
Traitement des Troubles Anxieux et de l’Humeur –
est un organisme de recherche indépendant dont les
membres sont issus de plusieurs universités
canadiennes. L’objectif final du CANMAT est
d’améliorer la qualité de vie des personnes souffrant
de troubles de l’humeur et de l’anxiété, par des
projets et des registres de recherches novatrices,
le développement de programmes d’éducation
fondés sur des données probantes et les meilleures
pratiques et l’élaboration de lignes
directrices/politiques.
CURRENT CLINICAL TOPICS FROM LEADING RA SPECIALISTS ACROSS CANADA AND AROUND THE
WORLD INVITED BY THE REBECCA MACDONALD CENTRE FOR ARTHRITIS AND AUTOIMMUNE DISEASE
UNE RESSOURCE ÉDUCATIVE POUR LES MÉDECINS DE L’ASSOCIATION CANADIENNE POUR LE TRAITEMENT DES TROUBLES ANXIEUX ET DE L’HUMEUR
2013 VOLUME 2, NUMÉRO 1
Association Canadienne pour le Traitement des
Troubles Anxieux et de l’Humeur
Disponible sur Internet à www.humeuretanxieteconferences.ca
Les troubles de
l’humeur et de l’anxiété
Conférences scientifiquesMD
Les troubles bipolaires (TB) font partie des affections que les cliniciens ont le plus de difficultés à traiter,
un défi que le CANMAT a tenté de relever par la publication de lignes directrices sur le traitement des TB
en 1997, 2005, 2007, 2009 et actuellement par une mise à jour 2013. Les lignes directrices initiales ont été
élaborées selon une méthodologie classique, notamment l’évaluation des données sur la base de critères
normalisés, ainsi que des recommandations cliniques incorporant une évaluation des éléments de preuve
avec un consensus clinique sur la faisabilité de la recommandation basée sur la tolérabilité et l’innocuité.
L’article complet comprend 8 sections portant sur toutes les phases des TB et sur d’autres thèmes clés. Dans
ce numéro de Les troubles de l’humeur et de l’anxiété – Conférences scientifiques, nous soulignons les élé-
ments les plus importants inclus dans la mise à jour de 2013 en mettant l’accent sur les modifications effec-
tuées. L’article principal de 2005 et la mise à jour de 2013, tous deux publiés dans la revue Bipolar
Disorders, comprennent des informations plus complètes et plus détaillées.
Introduction – Nouvelles données sur l’épidémiologie et les caractéristiques cliniques
Les trouble bipolaires (TB), incluant un spectre de sous-types, touchent jusqu’à 4 % de la population
générale1,2. Une étude de 61 392 individus provenant de 3 continents confirme largement les constatations ini-
tiales, révélant des taux au cours de la vie de 0,6 % pour le trouble bipolaire I (BP-I)a, de 0,4 % pour le TB-IIa
et de 1,4 % pour le TB infraliminaire3. Schaffer et ses collaborateurs4ont calculé un taux de prévalence pondéré
au cours de la vie de 2,2 % chez les Canadiens, et des taux réduits de prévalence et de traitement dans des pop-
ulations d’immigrants. Bulloch et ses collaborateurs5ont estimé que de 0,4 à 1,2 % de la population
Canadienne était traité par des psychiatres pour un TB-I. Dans l’ensemble, ces observations suggèrent que
d’importants progrès dans le diagnostic et le traitement des TB ont été effectués au Canada.
Les données démographiques et les caractéristiques cliniques significatives associées au diagnostic de TB
incluaient le jeune âge, un faible revenu, un diagnostic de trouble anxieux et l’abus de substances au cours des
12 mois précédents. L’âge moyen d’apparition chez les patients canadiens atteints d’un TB était de 22,5 ans4et
dans l’étude américaine NCS-R (National Comorbidity Survey Replication)1, l’âge moyen lors du premier
épisode maniaque/hypomaniaque ou du premier épisode dépressif majeur était de seulement 18,2 ans pour le
TB-I. Perlis et ses collaborateurs6ont constaté que chez 65,3 % des sujets (N = 983) recrutés dans le Systematic
Treatment Enhancement Program for Bipolar Disorder du National Institute of Mental Health, le TB est survenu
avant l’âge de 19 ans et chez 27,7 % avant l’âge de 13 ans. Kroon et ses collaborateurs7ont identifié 2 pics d’âge
d’apparition : 15 à 24 ans et 45 à 54 ans. Des antécédents parentaux de dépression majeure, de TB ou de schiz-
ophrénie peuvent réduire l’âge du premier épisode de 4 à 5 ans comparativement aux individus qui n’ont pas
de tels antécédents familiaux8.
Le taux d’affections médicales et psychiatriques concomitantes parmi les patients atteints de TB est très
élevé9. Les problèmes métaboliques et les troubles anxieux comptent parmi les plus courants et nécessitent des
stratégies thérapeutiques additionnelles, qui ont été décrites dans une série de rapports de groupes de travail
du Réseau canadien pour le traitement des troubles affectifs et de l’humeur (CANMAT)10-12.
Le TB est généralement un trouble qui dure toute la vie, caractérisé par un cycle de rémissions et de
rechutes. Il altère significativement de nombreux domaines fonctionnels, tels que les tâches quotidiennes, les
activités professionnelles et les activités sociales et de loisirs. Deux études récentes – EMBLEM13 en Europe et
UNITE14, une enquête internationale réalisée auprès de patients – soulignent les taux élevés d’incapacité au
travail, une majorité d’entre eux n’étant pas capables de conserver un emploi à plein temps. À la lumière de
ces difficultés, il n’est peut-être pas surprenant qu’une méta-analyse de 19 comparaisons intergroupes (N =
1838) réalisée par Nilsson et ses collaborateurs15 ait montré que l’estime de soi chez ces patients est faible,
même pendant les rémissions, ce qui indique une cible spécifique en psychothérapie. De plus, les patients
aVoir la sous-section sur la classification sous le titre Fondements du traitement pour les définitions du TB-I et du TB-II .

atteints de TB présentent un risque notablement élevé de suicide16-20.
Une méta-analyse de 15 études réalisée par Novick et ses collabora-
teurs16 a révélé des taux de prévalence de tentatives de suicide de 36,3
% dans le TB-I et de 32,4 % dans le TB-II. Tous ces facteurs soulig-
nent la complexité et la chronicité des TB, d’où la nécessité d’établir
un modèle systématique de prise en charge de ces maladies
chroniques qui serait appliqué par une équipe médicale multidisci-
plinaire. Toutes les versions des lignes directrices du CANMAT, inclu-
ant la mise à jour de 201321, ont souligné la nécessité d’un traitement
coordonné et multimodal, en mettant l’accent sur ses fondements,
comme conditions essentielles du succès du traitement de toutes les
phases du TB.
Fondements du traitement
Classification et diagnostic
Les TB sont divisés en 3 catégories22,23. Le TB-I est caractérisé par
la présence d’au moins un épisode maniaque complet, avec ou sans
dépression (bien que la plupart des personnes atteintes de TB-I souf-
frent de dépression). En revanche, le TB-II est caractérisé par un
tableau clinique regroupant des symptômes primaires de dépression
récurrente accompagnés d’épisodes hypomaniaques. Enfin, les trou-
bles bipolaires non classés ailleurs, appelés antérieurement TB non
spécifiés (NS), comprennent les troubles accompagnés de symptômes
maniaques/hypomaniaques qui ne répondent pas aux critères utilisés
pour les sous-types définis de TB, tels que l’élévation de l’humeur
mais où les symptômes sont trop peu nombreux ou une durée trop
courte de l’hypomanie. Dans tous les cas, pour être considérés comme
associés à un TB, ces tableaux clini ques doivent être exclusivement dus
à l’utilisation d’une substance, à une affection médicale ou à un
trouble psychiatrique concomitant.
Le nouveau Manuel diagnostique et statistique des troubles men-
taux, 5eédition (DSM-5) comprend des sections séparées sur les TB et
les affections associées, et les troubles dépressifs22,24. Le Critère A relatif
aux épisodes maniaques et hypomaniaques a été modifié de façon
importante, car il met désormais l’accent sur les modifications du
niveau d’activités/d’énergie et non pas uniquement sur les variations
de l’humeur. De plus, la catégorie « épisode mixte » considérée comme
une entité indépendante dans le DSM-IV a été éliminée. Désormais,
les épisodes sont caractérisés comme maniaques, hypomaniaques ou
dépressifs, avec l’ajout de la spécification « avec des caractéristiques
mixtes » en présence de symptômes significatifs du pôle opposé. Une
spécification additionnelle permet également l’évaluation des symp-
tômes d’anxiété concomitants.
Le respect des lignes directrices existantes, afin d’assurer l’identi-
fication exacte et le diagnostic différentiel des TB, plutôt que l’utilisa-
tion de moyens heuristiques, est une méthode efficace pour éviter un
diagnostic erroné25-27. Les observations de la famille, des aidants et/ou
des amis fournissent généralement des informations complémentaires
ou confirmant le diagnostic. De plus, les entrevues diagnostiques
manua lisées, telles que l’entrevue clinique structurée pour le DSM-IV
(ECS)28 et le Schedule for Affective Disorders and Schizophrenia
(SADS)29 ainsi que les tests de dépistage tels que le General Behavior
Inventory30 ou le Questionnaire sur les troubles de l’humeur (MDQ)31,
sont des instruments importants pour une évaluation complète. Le
journal personnel des patients est également utile comme moyen de
recueillir des informations diagnostiques.
Un facteur de nuisance clé est la prévalence élevée d’autres trou-
bles médicaux et psychiatriques, qui sont soit la cause sous-jacente des
symptômes de type bipolaire soit des comorbidités accompagnant
les TB. Les troubles de l’anxiété, de la personnalité et de l’utilisation
de substances sont les affections psychiatriques comorbides les plus
courantes, qui peuvent simuler les symptômes des TB. Le chevauche-
ment des symptômes entraîne souvent un diagnostic erroné32-34. Par
exemple, les changements au niveau de l’énergie, du sommeil et/ou de
l’irritabilité sont des caractéristiques d’une variété de troubles autres
que les TB, ce qui souligne l’importance d’un diagnostic différentiel
minutieux.
Traitement aigu de la manie bipolaire
Les épisodes de manie et d’hypomanie sont les manifestations
typiques des TB. L’interprétation des états typiques d’agitation dans
les épisodes maniaques aigus est un défi sur le plan diagnostique et
thérapeutique. La manie peut être pure ou mixte, c’est-à-dire accom-
pagnée de symptômes dépressifs intercurrents24. Le patient peut pré -
senter ou non des symptômes psychotiques (p. ex. les hallucinations
ou les idées erronées). Il peut également avoir des antécédents de
cycles rapides.
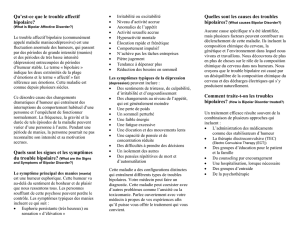
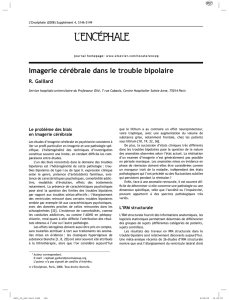
Un tableau clinique d’agitation et/ou d’agression nécessite une
évaluation initiale et un traitement urgents. L’algorithme de traite-
ment élaboré par le CANMAT pour la manie aiguë est illustré à la
figure 121. La pharmacothérapie pour la manie aiguë est appuyée par
plusieurs méta-analyses35-37. Les options de monothérapie de première
ligne demeurent les stabilisateurs de l’humeur comme le lithium et le
divalproex, et les antipsychotiques atypiques comme la rispéridone,
l’olanzapine, la quétiapine à libération standard ou prolongée (LS,
LP), la ziprasidone et l’aripiprazole. La mise à jour de 2013 a ajouté le
divalproex LP, l’asénapine et la palipéridone LP comme autres agents
de première ligne recommandés. Certaines caractéristiques cliniques
peuvent orienter les choix de médicaments chez un patient donné.
Par exemple, le lithium peut être plus efficace dans les cas de manie
euphorique classique, alors que dans les cas d’épisodes mixtes ou
d’antécédents de cycles rapides, le divalproex peut être plus favorable.
Les antipsychotiques atypiques peuvent être plus efficaces dans la
manie mixte et sont particulièrement préférés en présence d’agitation
ou de psychose. La combinaison d’un stabilisateur d’humeur et d’un
antipsychotique atypique, qui a été plus rapidement efficace et a pro-
duit des taux de réponses de 20 % plus élevés qu’un stabilisateur de
l’humeur seul38, est encore utilisé comme traitement de première ligne.
L’asénapine a été ajoutée aux combinaisons d’antipsychotiques aty pi-
ques à la suite de la publication des résultats d’une étude de prolonga-
tion de 40 semaines faisant suite à un essai randomisé et contrôlé
(ERC) démontrant une amélioration significative des symptômes de
manie comparativement à un placebo chez des patients recevant du
lithium/divalproex39. L’absence de réponse à un essai de 2 semaines
avec les agents ci-dessus devrait inciter à passer à un autre médica-
ment de première ligne ou à ajouter un deuxième médicament de pre-
mière ligne. On devrait faire l’essai de plusieurs options de première
ligne avant de passer à un médicament de deuxième ligne. L’utilisation
du clonazépam en concomitance est également fréquemment utile.
Dans la mise à jour de 2013, l’halopéridol a été ajouté aux options
antérieures de monothérapie de deuxième ligne – la carbamazépine
(standard et LP) et thérapie électroconvulsive (TEC). L’halopéridol est
utilisé désormais non plus en traitement de troisième ligne mais en
traitement de deuxième ligne sur la base d’une méta-analyse réalisée
par Cipriani et ses collaborateurs35 qui a révélé que ce médicament
présentait l’effet de taille le plus important dans le traitement de la
manie aiguë. La combinaison de médicaments de deuxième ligne
demeure le lithium + le divalproex. Les options de troisième ligne
destinées aux patients réfractaires au traitement, incluent l’addition
de la cariprazine en monothérapie ainsi que de la chlorpromazine, de
la clozapine et de l’oxcarbazépine. Cependant, la cariprazine n’a pas
été approuvée par Santé Canada. La mise à jour de 2013 recommande
également d’envisager d’utiliser des agents nouveaux/expérimentaux,
tels que la zotépine, le lévétiracétam, la phénytoïne, la mexilétine, les
acides gras Ω3, la calcitonine, un régime de déplétion rapide en tryp-
tophane, l’allopurinol, l’amisulpride, l’acide folique et la mémantine.
Traitement de la dépression dans
le trouble bipolaire I aigu
La dépression dans le TB est significativement plus courante que
la manie, et les patients atteints d’un TB sont beaucoup plus suscepti-
bles de demander une aide médicale pendant un épisode dépressif que
pendant un épisode maniaque40. Kupka et ses collaborateurs41 ont
établi des ratios de 2,9 pour la dépression/manie et de 3,8 pour le
TB-I et le TB-II, respectivement. La dépression bipolaire a également

un impact beaucoup plus profond sur les patients en termes de durée
et de qualité de vie, que les épisodes maniaques40.
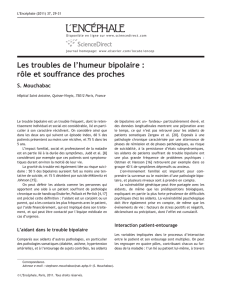
Les recommandations élaborées par le CANMAT pour le traite-
ment de la dépression dans le trouble bipolaire I sont classées dans
le tableau 121. Aucun changement n’a été apporté aux listes de
monothérapies de première ligne – lithium, lamotrigine et quétiapine
(standard et LP) – ou à la combinaison de médicaments de première
ligne (lithium ou divalproex + un inhibiteur sélectif des récepteurs de
la sérotonine [ISRS], olanzapine + ISRS, lithium + divalproex, lithium
ou divalproex + bupropion). La paroxétine ne doit pas être utilisée
dans les combinaisons mentionnées précédemment comme la com-
posante ISRS. Comme pour la manie bipolaire, il a été démontré que
l’absence de réponse précoce (2-3 semaines) suffit pour justifier le
passage à d’autres traitements.
Pour le traitement de deuxième ligne, la lurasidone a rejoint le
divalproex en monothérapie. L’utilisation de la lurasidone ou de la
lamotrigine combinée avec le lithium ou le divalproex est également
nouvelle. Le modafinil en traitement d’appoint et la quétiapine + un
ISRS représentent toujours des options de combinaisons de deuxième
ligne. Dans les études préliminaires, la lurasidone s’est montrée effi-
cace pour la dépression bipolaire en monothérapie et en traitement
d’appoint, mais l’absence d’expérience clinique et la non-
publication des versions finales des études clés réalisées en vue de
l’homo logation du médicament au moment de la rédaction des lignes
directrices du CANMAT n’ont pas permis de recommander la lurasi-
done comme traitement de première ligne42,43. Les monothérapies dans
les options de troisième ligne sont principalement les mêmes : carba-
mazépine, olanzapine et TEC. Il est important de noter que les
médicaments ajoutés dans la catégorie « non recommandé » inclu-
aient le lévétiracétam en traitement d’appoint et la ziprasidone, en
monothérapie ou en traitement d’appoint. Cette mise à jour reflète les
versions des lignes directrices antérieures identifiant le TEC comme
un choix potentiel en première ou en deuxième ligne dans certains
cas, en particulier pour la dépression bipolaire psychotique et en
présence d’un risque élevé de suicide et de complications médicales
dues au fait de ne pas manger ou boire21. Deux essais récents avec le
TEC confirment l’efficacité de ce traitement chez des patients atteints
d’un TB. On notera que chez les patients atteints d’un TB sous anti-
convulsivants, le TEC a été efficace, mais ils ont eu besoin d’un plus
grand nombre de séances de TEC que les patients atteints de TB
n’étant pas sous anticonvulsivants44,45. Les recommandations addition-
nelles de stratégies de troisième ligne incluent les combinaisons lithi-
um + carbamazépine, lithium + pramipexole, lithium ou divalproex +
venlafaxine, lithium + un inhibiteur de la monoamine oxydase
(IMAO) et lithium ou divalproex ou un antipsychotique atypique +
un antidépresseur tricyclique. Enfin, les lignes directrices incluent une
discussion nuancée sur les controverses relatives à l’utilisation des
antidépresseurs pour la dépression bipolaire, suggérant l’usage de
courte durée de la plupart des ISRS ou du bupropion conjointement à
un stabilisateur de l’humeur, en évitant la paroxétine, la venla faxine et
les antidépresseurs tricycliques.
Traitement d’entretien
Les cycles de rémissions-rechutes dans les TB soulignent l’impor-
tance d’un traitement d’entretien, et c’est durant cette phase que la
psychothérapie joue un rôle essentiel, comme nous le résumons ci-
dessous. Les facteurs associés au temps avant la survenue d’une
rechute incluent l’observance du traitement, la présence de symp-
tômes sous-syndromiques, le stress psycho -social de base, un nombre
plus élevé d’épisodes antérieurs, la présence d’un TB-II comparative-
ment à un TB-I, le sexe féminin, l’abus récent de substances et des
cycles rapides46-48. La rechute est souvent liée à l’inobservance médica-
menteuse qui selon les lignes directrices est associée à une fréquence
élevée d’épisodes bipolaires (surtout dépressifs), à des taux accrus
d’hospitalisation et de visites aux urgences et à un absentéisme au tra-
vail accru. La littérature rapporte des taux d’observance du traitement
pharmacologique prescrit de l’ordre de 70 % à seulement 31 %49-53. Les
facteurs qui augmentent l’inobservance incluent un manque de com-
préhension ou de sensibilisation au TB, les effets indésirables (EI),
l’inefficacité du traitement, une routine quotidienne/des conditions
Évaluer l’innocuité/le fonctionnement
Établir un plan de traitement
Arrêter les antidépresseurs
Exclure les causes médicales
Arrêter la consommation de caféine, d’alcool
et de substances illicites
Stratégies comportementales/rythmes,
psycho-éducation
Ne reçoit pas de
traitement ou d’agent
de 1
ère
intention
Sous agent 1
ère
intention
Aucune réponse
Aucune réponse
Aucune réponse
Initier : Li, DVP, APA
ou combinaison de
2 médicaments
Étape 1 :
Examiner les principes
généraux et évaluer
l’état de santé
Étape 2 :
Initier/optimiser,
vérifier l’observance
Étape 5 :
Ajouter des agents
nouveaux ou expérimentaux
Étape 3 :
Ajouter un médicament ou
passer à un autre médicament
Étape 4 :
Ajouter un médicament ou
passer à un autre médicament
Ajouter/passer
à un APA
Ajouter/passer
à Li ou DVP
Remplacer un ou les 2
agents par d’autres
agents de 1
ère
intention
Remplacer un ou les deux
agents par d’autres
agents de 1
ère
intention
Envisager d’ajouter ou
passer au deuxième
ou troisième agents
Envisager d’ajouter un agent
nouveau ou expérimental
Li
ou DVP
Combinaison de
2 médicaments
(Li ou DVP + APA)
APA
Figure 1 : Algorithme de traitement pour la manie aiguë
Li = lithium; DVP = divalproex; APA = antipsychotique atypique
Reproduit de Yatham LN et coll. Bipolar Disord. 2013;15(1):1-44. Copyright © 2012 John Wiley and Sons A/S.

Les troubles de
l’humeur et de l’anxiété
Conférences scientifiques
de vie irrégulières, des difficultés à prendre régulièrement ses
médicaments, la polarité dépressive du dernier épisode aigu,
l’utilisation concomitante de substances et la croyance par le
patient que ses médicaments ne sont plus nécessaires. Les com-
plications concernant les EI sont associées aux EI eux-mêmes
dont les patients font l’expérience (réels ou imaginés) et à la
peur des EI perçus. La sédation et le gain pondéral comptaient
parmi les effets secondaires les plus importants liés à une obser-
vance réduite49.
On n’a noté aucun changement dans les options de traite-
ment d’entretien : le lithium, la lamotrigine (efficace unique-
ment dans la prévention des rechutes de dépression), le dival-
proex, l’olanzapine, la quétiapine, la rispéridone injectable à
action prolongée (IAP) et l’aripiprazole. Les combinaisons de
médicaments de première ligne demeurent le lithium ou le
divalproex + la quétiapine, la rispéridone IAP, l’aripiprazole ou
la ziprasidone. Il existe toujours des preuves convaincantes de
l’efficacité du lithium, de la lamotrigine, de l’olanzapine et (dans
une moindre mesure) du divalproex. Il existe un écart au niveau
des éléments de preuve pour la phase d’entretien, étant donné
que la plupart des ERC ont une durée ≤ 1 an et aucun n’a une
durée supérieure à 2 ans. Néanmoins, 2 méta-analyses54,55 résu-
ment les données existantes, afin de démontrer l’efficacité des
traitements d’entretien de première et de deuxième ligne dans
les lignes directrices du CANMAT.
En ce qui concerne le traitement de deuxième ligne, la
palidéridone LP a été ajoutée à la carbamazépine en mono théra -
pie. Les combinaisons de médicaments demeurent in changées
par rapport à la mise à jour de 2009 : lithium avec l’un des agents
sui vants : divalproex, carbamazépine, olanzapine, rispéridone ou
lamotrigine, divalproex + olanzapine et olanzapine + fluoxétine.
La nouvelle option pour le traitement de troisième ligne est l’asé-
napine, en monothérapie et en traitement d’appoint, qui a été
ajoutée sur la base de nouvelles données publiées montrant des
effets bénéfiques56,57. D’autres options de traitement d’appoint
incluent la phénytoïne, la clozapine, le TEC, le topiramate, les
acides gras Ω-3, l’oxcarbazépine et la gabapentine.
Psychothérapie
La littérature a appuyé historiquement les effets bénéfiques
des interventions psychologiques – incluant la psychoéducation,
la thérapie cognitivo-comportementale (TCC), la thérapie
familiale et la psychothérapie interpersonnelle et des rythmes
sociaux – combinées avec une pharmacothérapie. Lam et ses col-
laborateurs58 ont conclu que les psychothérapies étaient efficaces
dans la prévention ou le retardement des rechutes (risque relatif
global 0,74; intervalle de confiance à 95 % 0,64 à 0,85). Plusieurs
études ont fourni des données contradictoires sur la valeur de la
TCC pour le TB59-62, mais 2 autres études63,64 ont souligné l’effi-
cacité de la psychoéducation seule ou comme composante de la
TCC, et l’on a noté un excellent rapport coût-efficacité pour la
psychoéducation de groupe.
La psychoéducation doit être administrée lorsque le diag-
nostic de TB est établi pour la première fois, mais une réitération
et un renforcement périodique de courte durée sont nécessaires :
la répétition complète (des années après le diagnostic) d’un pro-
gramme psycho-éducatif en mettant l’accent sur un exercice de
prévention des rechutes est souvent utile.
Traitement aigu et traitement d’entretien
du trouble bipolaire II
Comme nous l’avons mentionné antérieurement, le TB-II
est caractérisé par la phénoménologie d’épisodes de dépression
et d’hypomanie : les premiers, syndromiques ou sous-syndro -
miques, sont la caractéristique principale du TB-II22,23. Le TB-II
est considéré comme la forme dont la prévalence est la plus
élevée, et les cycles rapides peuvent être plus fréquents que dans
le TB-I23,65,66. L’absence d’études bien conçues sur le TB-II con-
stitue un obstacle à l’élaboration de recommandations fondées
sur des données probantes pour l’hypomanie. Les lignes direc-
trices actuelles sont donc fondées sur l’extrapolation de
thérapies efficaces pour la manie sur la base de l’expérience clin-
ique accumulée.
Peu de changements ont été apportés aux recommanda-
tions sur le traitement de la dépression aiguë dans le TB-II
figurant dans les lignes directrices mises à jour. La quétiapine
demeure l’unique monothérapie de première ligne. La forme LP
a été ajoutée à la forme standard. Le traitement de deuxième
ligne est identique à celui prescrit dans la mise à jour précédente :
lithium, lamotrigine, divalproex, lithium ou divalproex + anti-
dépresseurs, lithium + divalproex + antidépresseurs et antipsy-
chotiques atypiques + antidépresseurs. Les nouvelles options
pour le traitement de troisième ligne incluent la quétiapine + la
lamotrigine et une TEC d’appoint, la N-acétylcystéine ou la tri-
iodothyronine, qui ont été ajoutées à la monothérapie par des
antidépresseurs (principalement pour ceux présentant des
hypomanies peu fréquentes) et d’autres antidépresseurs.
Tableau 1 : Recommandations pour la traitement
pharmacologique de la dépression dans le trouble
bipolaire I aigua
Première ligne
Monothérapie Lithium, lamotrigine, quétiapine,
quétiapine LP
Thérapie de Lithium ou divalproex + ISRSb,
olanzapine + ISRSb, lithium +
divalproex, lithium ou divalproex
+ bupropion
Deuxième ligne
Monothérapie Divalproex, lurasidonec
Thérapie de Quétiapine + ISRSb, modafinil en
traitement d’appoint, lithium ou
divalproex + lamotriginec, lithium
ou divalproex + lurasidonec
Troisième ligne
Monothérapie Carbamazépine, olanzapine, TECd
Thérapie de Lithium + carbamazépine,
lithium + pramipexole, lithium ou
divalproex + venlafaxine, lithium +
IMAO, lithium ou divalproex ou
APA + ATC, lithium ou divalproex
ou carbamazépine + ISRSb+
lamotrigine, quétiapine +
lamotriginec
Non recommandé
Monothérapie Gabapentine, aripiprazole,
ziprasidonec
Thérapie de Ziprasidonecou levetiracetamc
en traitement d’appoint
TEC = thérapie électroconvulsive; IMAO = inhibiteur de la monoamine
oxydase; ATC = antidépresseur tricyclique; ISRS = inhibiteur sélectif des
récepteurs de la sérotonine; LP = libération prolongée.
aLe traitement d’un épisode dépressif bipolaire avec des antidépresseurs
demeure complexe. Le clinicien doit faire la part des choses entre l’effet
désiré de la rémission et l’effet indésirable du passage à un autre
médicament.
bExcepté la paroxétine.
cNouveau ou changement conformément aux recommandations.
dPourrait être utilisé comme traitement de première et de deuxième
intention dans certaines situations.
Reproduit de Yatham LN et coll. Bipolar Disord. 2013;15(1):1-44.
Copyright © 2012 John Wiley and Sons A/S.
combinaison
combinaison
combinaison
combinaison

En ce qui concerne le traitement d’entretien pour le TB-II,
la quétiapine a été ajoutée aux options existantes de première
ligne, i.e. le lithium et la lamotrigine. La quétiapine et la lamo-
trigine en traitement d’appoint sont les nouveaux éléments
dans le traitement de deuxième ligne, rejoignant le divalproex,
la combinaison lithium ou divalproex ou un antipsychotique
atypique + un antidépresseur et la combinaison de 2 des
médicaments suivants : lithium, divalproex ou un antipsycho-
tique atypique. La fluoxétine est la dernière option de troisième
ligne avec la carbamazépine, l’oxcarbazépine, les antipsycho-
tiques atypiques et le TEC.
Conclusion
La mise à jour 2013 des lignes directrices élaborées par le
CANMAT met à nouveau en lumière les approches diagnos-
tiques et thérapeutiques adoptées à l’égard de l’important prob-
lème de santé à l’échelle mondiale que posent les TB et fournit
de nouvelles options thérapeutiques efficaces pour les diverses
composantes et les divers tableaux cliniques des TB. Les
thérapies doivent être adaptées à chaque patient, idéalement
avec des composantes pharmacologiques et psychothérapeu-
tiques et une évaluation complète régulière du patient, afin de
maximiser l’issue et l’innocuité du traitement. En raison de con-
traintes d’espace, cet article ne résume que les sections sur les
fondements de la prise en charge et sur le traitement de chaque
phase du TB. La mise à jour complète 2013 des lignes directrices
incluent des sections additionnelles précieuses sur les popula-
tions spéciales comme les femmes, les enfants et les personnes
âgées, sur le trouble bipolaire II et sur la surveillance
métabolique. L’article complet ainsi que les versions antérieures
des lignes directrices peuvent être téléchargés à partir du site
Web du CANMAT à l’adresse www.canmat.org.
Le DrParikh est professeur de psychiatrie à l’Université de
Toronto et psychiatre en chef adjoint au sein du Réseau univer-
sitaire de santé, Toronto, Ontario. Le DrGoldstein est professeur
adjoint de psychiatrie et de pharmacologie à l’Université de
Toronto et professeur adjoint associé de psychiatrie à l’Université
de Pittsburgh. Il est directeur du Centre for Youth Bipolar
Disorder au Centre des sciences de la santé Sunnybrook et
chercheur au Sunnybrook Research Institute, Toronto, Ontario.
Références :
11. Merikangas KR, Akiskal HS, Angst J, et coll. Lifetime and 12-month prevalence
of bipolar spectrum disorder in the National Comorbidity Survey Replication.
Arch Gen Psychiatry. 2007;64(5):543-552.
12. Hirschfeld RM, Calabrese JR, Weissman MM, et coll. Screening for bipolar
disorder in the community. J Clin Psychiatry. 2003;64(1):53-59.
13. Merikangas KR, Jin R, He JP et coll. Prevalence and correlates of bipolar
spectrum disorder in the world mental health survey initiative. Arch Gen
Psychiatry. 2011;68(3):241-251.
14. Schaffer A, Cairney J, Cheung A, Veldhuizen S, Levitt A. Community survey of
bipolar disorder in Canada: lifetime prevalence and illness characteristics.
Can J Psychiatry. 2006;51(1):9-16.
15. Bulloch AG, Currie S, Guyn L, Williams JV, Lavorato DH, Patten SB. Estimates
of the treated prevalence of bipolar disorders by mental health services in the
general population: comparison of results from administrative and health
survey data. Chronic Dis Inj Can. 2011; 31(3):129-134.
16. Perlis RH, Miyahara S, Marangell LB, et coll; STEP-BD Investigators. Long-
term implications of early onset in bipolar disorder: data from the first 1000
participants in the systematic treatment enhancement program for bipolar
disorder (STEP-BD). Biol Psychiatry. 2004;55(9): 875-881.
17. Kroon JS, Wohlfarth TD, Dieleman J, et coll. Incidence rates and risk factors of
bipolar disorder in the general population: a population-based cohort study.
Bipolar Disord. 2013;15(3):306-313.
18. Chengappa KN, Kupfer DJ, Frank E, et coll. Relationship of birth cohort and
early age at onset of illness in a bipolar disorder case registry. Am J Psychiatry.
2003;160(9): 1636-1642.
19. McIntyre RS, Rosenbluth M, Ramasubbu R, et coll; Canadian Network for
Mood and Anxiety Treatments (CANMAT) Task Force. Managing medical and
psychiatric comorbidity in individuals with major depressive disorder and
bipolar disorder. Ann Clin Psychiatry. 2012; 24(2):163-169.
10. Ramasubbu R, Beaulieu S, Taylor VH, Schaffer A, McIntyre RS; CANMAT Task
Force. The CANMAT task force recommendations for the management of
patients with mood disorders and comorbid medical conditions: diagnostic,
assessment, and treatment principles. Ann Clin Psychiatry. 2012;24(1):82-90.
11. McIntyre RS, Alsuwaidan M, Goldstein BI, et coll; CANMAT Task Force. The
Canadian Network for Mood and Anxiety Treatments (CANMAT) task force
recommendations for the management of patients with mood disorders and
comorbid metabolic disorders. Ann Clin Psychiatry. 2012;24(1): 69-81.
12. Schaffer A, McIntosh D, Goldstein BI, et coll; CANMAT Task Force. The CAN-
MAT task force recommendations for the management of patients with mood
disorders and comorbid anxiety disorders. Ann Clin Psychiatry. 2012;24(1):
6-22.
13. Reed C, Goetz I, Vieta E, Bassi M, Haro JM; EMBLEM Advisory Board. Work
impairment in bipolar disorder patients–results from a two-year observational
study (EMBLEM). Eur Psychiatry. 2010;25(6):338-344.
14. McIntyre RS. Understanding needs, interactions, treatment, and expectations
among individuals affected by bipolar disorder or schizophrenia: the UNITE
global survey. J Clin Psychiatry. 2009;70(Suppl. 3):5-11.
15. Nilsson KK, Jørgensen CR, Craig TKJ, Straarup KN, Licht RW. Self-esteem in
remitted bipolar disorder patients: a meta-analysis. Bipolar Disord. 2010;12(6):
585-592.
16. Novick DM, Swartz HA, Frank E. Suicide attempts in bipolar I and bipolar II
disorder: a review and meta-analysis of the evidence. Bipolar Disord. 2010;
12(1):1-9.
17. Clements C, Morriss R, Jones S, Peters S, Roberts C, Kapur N. Suicide in bi-
polar disorder in a national English sample, 1996-2009: frequency, trends and
characteristics. Psychol Med. 2013 19 mars:1-10. [Publication électronique
avant impression]
18. Goldstein TR, Ha W, Axelson DA, et coll. Predictors of prospectively examined
suicide attempts among youth with bipolar disorder. Arch Gen Psychiatry.
2012;69(11):1113-1122.
19. Marangell LB, Bauer MS, Dennehy EB, et coll. Prospective predictors of
suicide and suicide attempts in 1,556 patients with bipolar disorders followed
for up to 2 years. Bipolar Disord. 2006;8(5 pt 2):566-575.
20. Valtonen HM, Suominen K, Mantere O, Leppämäki S, Arvilommi P, Isometsä
ET. Prospective study of risk factors for attempted suicide among patients with
bipolar disorder. Bipolar Disord. 2006;8(5 Pt 2):576-585.
21. Yatham LN, Kennedy SH, Parikh SV, et coll. Canadian Network for Mood and
Anxiety Treatments (CANMAT) and International Society for Bipolar
Disorders (ISBD) collaborative update of CANMAT guidelines for the
management of patients with bipolar disorder: update 2013. Bipolar Disord.
2013;15(1):1-44.
22. American Psychiatric Association. Diagnostic and Statistical Manual of Mental
Disorders, 5eédition. Arlington (VA): American Psychiatric Association Press;
2013.
23. Ghaemi SN, Bauer M, Cassidy F, et coll; ISBD Diagnostic Guidelines Task
Force. Diagnostic guidelines for bipolar disorder: a summary of the
International Society for Bipolar Disorders Diagnostic Guidelines Task Force
Report. Bipolar Disord. 2008;10(1 Pt 2):117-128.
24. National Institute of Mental Health. Bipolar Disorder. Bethesda (MD):
National Institutes of Health; révisé 2008. NIH Publication 08-3679.
Disponible à : http://www.nimh.nih.gov/health/publications/bipolar-disor-
der/complete-index.shtml. Date de consultation : 24 avril 2013.
25. Meyer F, Meyer TD. The misdiagnosis of bipolar disorder as a psychotic
disorder: some of its causes and their influence on therapy. J Affect Disord.
2009;112(1-3):174-183.
26. Wolkenstein L, Bruchmüller K, Schmid P, Meyer TD. Misdiagnosing bipolar dis-
order—do clinicians show heuristic biases? J Affect Disord. 2011;130(3): 405-412.
27. Bruchmüller K, Meyer TD. Diagnostically irrelevant information can affect the
likelihood of a diagnosis of bipolar disorder. J Affect Disord. 2009; 116(1-2):
148-151.
28. Spitzer RL, Williams JB, Gibbon M, First MB. The Structured Clinical
Interview for DSM-III-R (SCID). I: History, rationale, and description. Arch
Gen Psychiatry. 1992; 49(8):624-629.
29. Endicott J, Spitzer RL. A diagnostic interview: the schedule for affective disor-
ders and schizophrenia. Arch Gen Psychiatry. 1978;35(7):837-844.
30. Mallon JC, Klein DN, Bornstein RF, Slater JF. Discriminant validity of the General
Behavior Inventory: An outpatient study. J Pers Assess. 1986;50(4):568-577.
31. Hirschfeld RMA, Williams JBW, Spitzer RL, et coll. Development and valida-
tion of a screening instrument for bipolar spectrum disorder: The Mood
Disorder Questionnaire. Am J Psychiatry. 2000;157(11):1873-1875.
32. Sherwood Brown E, Suppes T, Adinoff B, Rajan Thomas N. Drug abuse and
bipolar disorder: comorbidity or misdiagnosis? J Affect Disord. 2001;65(2):105-
115.
33. Zimmerman M, Ruggero CJ, Chelminski I, Young D. Is bipolar disorder over-
diagnosed? J Clin Psychiatry. 2008;69(6):935-940.
34. Goldberg JF, Garno JL, Callahan AM, Kearns DL, Kerner B, Ackerman SH.
Overdiagnosis of bipolar disorder among substance use disorder inpatients
with mood instability. J Clin Psychiatry. 2008;69(11):1751-1757.
35. Cipriani A, Barbui C, Salanti G et coll. Comparative efficacy and acceptability
of antimanic drugs in acute mania: a multiple-treatments meta-analysis.
Lancet. 2011; 378(9799):1306-1315.
36. Correll CU, Sheridan EM, DelBello MP. Antipsychotic and mood stabilizer effi-
cacy and tolerability in pediatric and adult patients with bipolar I mania: a
comparative analysis of acute, randomized, placebo-controlled trials. Bipolar
Disord. 2010;12(2): 116-141.
Les troubles de
l’humeur et de l’anxiété
Conférences scientifiques
 6
6
1
/
6
100%