Médecine des maladies Métaboliques - Juin 2012 - Vol. 6 - N°3
Pour la pratique
220
© 2012 - Elsevier Masson SAS - Tous droits réservés.
Correspondance:
Mathilde Gallice
Service d’ophtalmologie
CHU de Grenoble
BP 217
38043 Grenoble cedex 9
M.Gallice1, C.Chiquet1,
J.-P.Romanet1, S.Halimi2
1 Service d’ophtalmologie, CHU de Grenoble;
Université Joseph Fourier, Grenoble.
2 Clinique endocrinologie-diabète-nutrition,
Pôle DigiDUNE, CHU de Grenoble;
Université Joseph Fourier,
Grenoble.
Rétinopathie diabétique
et hypertension artérielle
Diabetic retinopathy and hypertension
Résumé
La rétinopathie diabétique est la complication de microangiopathie la plus spécifique
liée aux diabètes. Le retentissement de l’hypertension artérielle (HTA) n’est pas limité
aux gros vaisseaux, mais porte également sur la rétinopathie et la maculopathie dia-
bétique. Nous décrivons les caractéristiques de l’HTA chez le patient diabétique de
type 1 par rapport au diabétique de type 2, ainsi que son action sur la rétinopathie.
Le contrôle tensionnel s’inscrit ainsi dans une prise en charge globale, afin de ralentir
l’apparition et la progression de la rétinopathie.
Mots-clés: Diabète –hypertension artérielle– rétinopathie diabétique –
œdème maculaire.
Summary
Diabetic retinopathy is the most specific microangiopathy related to diabetes.
Furthermore, hypertension is frequently associated with diabetes. The impact of hyper-
tension on large vessels is well known, but it has a deleterious effect on retinopathy
and diabetic maculopathy also. We describe the characteristics of this hypertension
in subjects with type 1 diabetes compared to type 2 diabetes and its effect on retino-
pathy. Blood pressure control is part of a comprehensive care to slow the onset and
progression of diabetic retinopathy.
Key-words: Diabetes –hypertension– diabetic retinopathy –macular edema.
Introduction
La rétinopathie diabétique (RD) consti-
tue la plus spécifique des complications
de microangiopathie liée aux diabètes.
Après 15ans d’évolution, 80% des
patients diabétiques peuvent être tou-
chés, à des degrés divers, par cette
complication. Toutefois, sa prévalence
diminue depuis que la prise en charge
des patients diabétiques a été consi-
dérablement améliorée. Dans les pays
industrialisés, elle demeure cependant
l’une des causes principales de cécité et
de malvoyance: environ 10% des dia-
bétiques souffrent de malvoyance après
15ans d’évolution de leur diabète[1, 2].
Par conséquent, la RD peut affecter le
patient dans sa vie quotidienne. Au-delà
des effets sur la qualité de vie et l’auto-
nomie des patients, les conséquences
sur la morbi-mortalité d’une telle baisse
de vision peuvent se traduire par l’aug-
mentation du nombre de chutes et de
fractures, de plaies et de troubles de
cicatrisation[3].

221
Rétinopathie diabétique et hypertension artérielle
Médecine des maladies Métaboliques - Juin 2012 - Vol. 6 - N°3
221
Le lien entre contrôle glycémique et réti-
nopathie est établi dans les deux princi-
pales formes de diabète:
− dans le diabète de type 1 (DT1), par
l’étude Diabetes control and compli-
cations trial (DCCT)[4] et son suivi,
Epidemiology of diabetes interventions
and complications (EDIC)[5];
− dans le diabète de type 2 (DT2), par
les études United Kingdom prospective
diabetes study (UKPDS)[6] et japonaise
de Kumamoto[7].
D’autres facteurs sont connus pour
aggraver le risque de progression de la
RD, au premier rang desquels, l’hyper-
tension artérielle (HTA). L’HTA est fré-
quemment associée au diabète. Les
questions clés qui en découlent sont:
− le contrôle tensionnel peut-il ralentir la
progression de la rétinopathie?
− faudrait-il initier un traitement antihyper-
tenseur à tout patient normotendu dia-
bétique, afin de protéger la rétine, tout
comme on l’envisage pour protéger le
rein?
L’hypertension artérielle
du diabétique
L’HTA est un problème de santé publique
majeur, qui touche toutes les popula-
tions, et, plus encore, les sujets diabé-
tiques[8, 9]! La prévalence de l’HTA chez
les patients diabétiques varie en fonction
de la définition de l’HTA employée:
− dans l’étude UKPDS, 39% des patients
diabétiques étaient hypertendus (pres-
sion artérielle[PA] >160/90mm Hg);
− dans l’étude Survey in diabetic adults in
England, 80% des patients diabétiques
étaient hypertendus (PA>140/90mmHg).
En France, l’objectif tensionnel chez le
patient diabétique est, actuellement, fixé
à 130mm Hg pour la PA systolique et
80mm Hg pour la PA diastolique[10],
voire un peu inférieur.
Cependant, l’HTA du DT1 et celle du DT2
sont deux entités dont l’histoire naturelle
est différente. Alors que l’apparition de
l’HTA est précoce, et peut même pré-
céder le diabète (HTA métabolique ou
vasculaire) chez le DT2, elle est, le plus
souvent, secondaire à la néphropathie
diabétique chez le DT1[11]. Ainsi, 35 à
60% des patients DT2 présentent une
HTA lors du diagnostic du diabète[12],
contrairement aux DT1 qui, générale-
ment, ne révèlent une HTA qu’après plu-
sieurs années d’évolution de leur diabète.
L’association diabète-HTA est aujourd’hui
reconnue pour aggraver le risque de
complication cardiovasculaire (corona-
ropathie, accident vasculaire cérébral,
décès), mais elle est également un fac-
teur majeur de complications microan-
giopathiques, telles que la néphropathie
et la rétinopathie.
Mécanismes aboutissant
à la rétinopathie diabétique
Physiopathologie
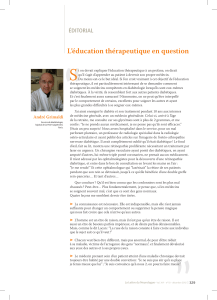
L’hyperglycémie chronique entraîne, via
des mécanismes cellulaires, enzyma-
tiques et vasculaires complexes, des
occlusions microvasculaires (figure1).
C’est sur ce terrain d’ischémie rétinienne
que se développe une néo-vascularisa-
tion rétinienne.
Facteurs aggravants
Plusieurs facteurs sont connus pour
aggraver le risque de progression de la
RD[13]:
− l’élévation de la pression artérielle;
− la durée d’évolution du diabète;
− l’hyperglycémie chronique;
− la dyslipidémie;
− l’anémie.
Vaisseaux rétiniens
du sujet hypertendu
La vascularisation rétinienne est une
vascularisation de type terminal, sans
innervation sympathique. Ainsi, en cas
d’élévation de la PA, la réponse vas-
culaire dépend de l’autorégulation. En
cas d’HTA, des anomalies vasculaires
rétiniennes s’installent, soit sur un
mode aigu, soit sur un mode chronique,
comme le précise la classification de
Kirkendall[14] (tableau I).
Figure1: Facteurs aboutissant à la néo-angiogenèse et à l’œdème maculaire dans le cadre du
diabète. NO : monoxyde d'azote.
DIABÈTE
HYPERGLYCÉMIE
CHRONIQUE
OCCLUSION
MICROVASCULAIRE
RUPTURE DE LA BARRIÈRE
HÉMATORÉTINIENNE
ŒDÈME MACULAIRE
Réponse
inammatoire
Activation de la VOIE DU SORBITOL
Activation de LA GLYCATION produit
de la glycation
MODIFICATIONS CELLULAIRES :
les cellules endothéliales dissocient
leurs jonctions serrées ; aggrégation ;
perte des péricytes
Production de FACTEURS DE CROISSANCE
Modications
du ux sanguin
rétinien ;
libération de NO
rétinien
Hypoxie rétinienne
NÉOANGIOGENÈSE

222 Pour la pratique
Médecine des maladies Métaboliques - Juin 2012 - Vol. 6 - N°3
Pour la pratique
222
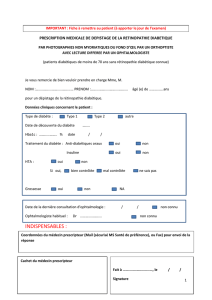
Le signe du croisement artério-veineux
est un reflet de lésion d’artériosclérose
(figure2). Les vaisseaux rétiniens cir-
culent dans une gaine adventicielle
commune au niveau des croisements
artério-veineux. Ainsi, l’épaississe-
ment de la paroi artérielle comprime
la veine, la faisant apparaître de plus
petit calibre et dilatée en amont. L’on
comprend bien que cet effet influence
la circulation du sang dans la veine cor-
respondante.
Rétinopathie hypertensive
Seuls 9% des patients hypertendus
présentent une rétinopathie hyperten-
sive[15]; elle est d’autant plus fréquente
que les patients présentent un mauvais
contrôle tensionnel.
La rétinopathie hypertensive peut s’as-
socier à la rétinopathie diabétique. La
rétinopathie hypertensive est le plus sou-
vent asymptomatique; elle est en général
bilatérale.
Différentes classifications ont été pro-
posées, reposant sur l’analyse du fond
d’œil. La classification de Kirkendall
distingue la rétinopathie hypertensive
en cas d’élévation aiguë de la PA et les
modifications chroniques[14] (tableau I).
L’intérêt de la classification de Wong et
Mitchell[16] est essentiellement pro-
nostique: le risque d’événement car-
diovasculaire grave (morbi-mortalité
cardiovasculaire) est associé à la gravité
de la rétinopathie hypertensive (tableauII).
Rétinopathie diabétique
et hypertension artérielle
Le contrôle tensionnel
ralentit la progression de la RD
Des études épidémiologiques ont mon-
tré que l’HTA est un facteur de risque
d’apparition[17, 18] et de progres-
sion[19] de la RD. L’étude UKPDS a
prouvé qu’une réduction de 10mm Hg
de PA systolique et de 5mm Hg de
PA diastolique (objectifs de PA systo-
lique <150mm Hg et de PA diasto-
lique <85mm Hg) réduisait le risque
de progression de la RD de 34% à
9ans. Lors de l’étude STENO2[20],
après 7,3ans, le risque de RD était
réduit dans le groupe bénéficiant d’un
traitement intensif, avec un objectif de
PA <130mm Hg pour la PA systolique
et <80mm Hg pour la PA diastolique
(risque relatif, RR =0,42[intervalle de
confiance à 95%, IC 95% 0,21-0,86] ;
p =0,02).
Cependant, en dessous d’un certain
seuil tensionnel, il n’est plus retrouvé
de différence significative dans la pro-
gression de la RD. Ainsi, l’étude Action
to control cardiovascular risk in dia-
betes (ACCORD)-Eye[21] ne retrouvait
pas de différence significative avec
un traitement antihypertenseur inten-
sif ayant pour objectif une PA systo-
lique<120mm Hg. De même, l’essai
ABCD (Appropriate blood control pres-
sure in diabetes)[22] n’a pas mis en
évidence de différence significative
entre une PA à 138/86mm Hg versus
132/78mm Hg sur la progression de
la RD.
Ainsi, le contrôle rigoureux de la PA
retarde l’apparition de la RD et ralentit
sa progression.
L’effet du contrôle de la PA
systolique et diastolique
• L’élévation initiale de la PA systo-
lique constitue un facteur prédictif d’in-
cidence de la RD: elle est associée à
Figure2: Signe du croisement artério-veineux (en encadré sur la photo): reflet de lésion d’ar-
tériosclérose.
Tableau I: Artériosclérose rétinienne selon
la classification de Kirkendall[14].
Stade I Signe du croisement
artério-veineux
Stade II Stade I associé
à un rétrécissement
artériolaire
Stade III Signes de pré-
occlusions veineuses
Tableau II: Classification de la rétinopathie hypertensive proposée par Wong et Mitchell[16].
Minime Modérée Sévère
Rétrécissement du calibre artériolaire
Signe du croisement
Rétinopathie minime +hémorragies/nodules cotonneux Rétinopathie modérée +œdème papillaire
Touche les artérioles Touche les capillaires Touche le nerf optique

223
Rétinopathie diabétique et hypertension artérielle
Médecine des maladies Métaboliques - Juin 2012 - Vol. 6 - N°3
223
Maculopathie diabétique
et hypertension artérielle
Œdème maculaire,
cause la plus fréquente
de baisse d’acuité visuelle
du diabétique
L’œdème maculaire est lié à l’hyper-
perméabilité capillaire qui engendre une
accumulation de liquide extracellulaire au
niveau de la macula. Il peut exister seul,
ou associé à la rétinopathie. Il concerne
plus volontiers les patients atteints d’un
DT2 et touche environ 26% des patients
DT2 insulino-traités (versus 14% des
DT2 non insulino-traités) et 20% des
patients DT1, après 10ans d’évolution
de leur diabète[32].
Toutes les classifications distinguent
l’œdème maculaire et la maculopathie
ischémique.
HTA, facteur de risque
reconnu de développement
d’œdème maculaire
Les traitements aujourd’hui employés
sont dirigés vers la maculopathie œdé-
mateuse. L’efficacité des moyens thé-
rapeutiques employés pour l’œdème
maculaire est assez limitée. Ainsi, la
prévention de son apparition est pri-
mordiale.
Lors de l’étude UKPDS, portant sur
des patients DT2, une cible de PA sys-
tolique <150mm Hg et de PA diasto-
lique <85mm Hg, a permis de réduire
la perte visuelle de 47% (p =0,004), par
réduction de l’œdème maculaire, après
8,4ans[12]. Plusieurs études ont mon-
tré l’effet protecteur du contrôle de la
PA diastolique sur l’œdème maculaire,
tant chez les diabétiques à début pré-
coce que chez les diabétiques à début
tardif[25, 33].
Conflits d’intérêt
Les auteurs ont déclaré n’avoir aucun conflit
d’intérêt en lien avec cet article.
Références
[1] Organisation mondiale de la santé (OMS).
Diabète sucré. www.who.int/mediacentre/
factsheets/fs138/fr/index.html
[2] Massin P. Complications oculaires du dia-
bète: uniformiser le dépistage et les soins.
Complications du diabète au long cours. Rev Prat
2001;51:1776-82.
diabétique normotendu (-35% chez le
DT1 en prévention primaire; régres-
sion significative, de 34%, en pré-
vention secondaire; études DIabetic
Retinopathy Candesartan Trials
(DIRECT)[29]).
De plus, l’étude EURODIAB controlled
trial of lisinopril in insulin-dependent dia-
betes (EUCLID)[30] a mis en évidence
un bénéfice significatif à employer un
inhibiteur de l’enzyme de conversion
de l’angiotensine (IEC) comme antihy-
pertenseur: réduction significative de
50% de la progression de la RD, chez
des patients DT1, après 2ans de traite-
ment par le lisinopril. Toutefois, il reste à
savoir si cet effet de moindre progression
de la RD était lié à la baisse de la PA
systolique (de 3mm Hg dans le groupe
traité), ou bien à un effet propre sur le
système rénine-angiotensine agissant au
niveau rétinien?
Effet des inhibiteurs calciques
et des E-bloquants (sélectifs)
Lors des essais cliniques, il n’a pas été
montré de supériorité dans l’efficacité
de ces molécules comparées à un inhi-
biteur du système rénine-angiotensine
(ABCD[22], UKPDS[31]).
Les effets d’une prise en charge
globale…
Au cours de l’essai STENO 2[20], la
prise en charge intensive de l’ensemble
des facteurs de risque cardiovasculaire
a permis de réduire, de 58%, le risque
de RD à 7ans chez le DT2 à haut risque
(RR: 0,42[IC 95% 0,21-0,86]).
l’augmentation du risque de RD chez
le patient DT2[23] et à la progression
vers la RD proliférante chez le patient
DT1[24].
• L’élévation de la PA diastolique
constitue un facteur prédictif de pro-
gression de la RD vers la RD prolifé-
rante[24, 25].
Les médicaments
antihypertenseurs à employer
Effets de l’inhibition du système
rénine-angiotensine
Le système rénine-angiotensine consti-
tue une cascade enzymatique capable
de réguler la PA. Les inhibiteurs du sys-
tème rénine-angiotensine ont été testés
pour plusieurs raisons, et tout d’abord en
raison de la physiologie: l’endothélium
rétinien exprime l’enzyme de conversion
de l’angiotensine à sa surface; stimu-
lée, elle entraîne une hyperproduction
du facteur de croissance de l’endothé-
lium vasculaire (vascular endothelial
growth factor, VEGF) chez le patient
diabétique. Le VEGF est un facteur de
prolifération vasculaire impliqué dans
la néo-angiogenèse. Plusieurs raisons
expérimentales le confirment: l’utilisa-
tion du candésartan (un antagoniste des
récepteurs de l’angiotensineII, ARA II)
permet une diminution de la production
de VEGF rétinien, entraînant une dimi-
nution de la néo-vascularisation chez
le souriceau nouveau-né[26] et chez le
rat[27, 28].
Le candésartan (32mg/jour) retarde et
ralentit la progression de la RD chez le
•L’hypertension artérielle (HTA) est souvent présente chez les sujets atteints de diabète.
•L’HTA joue un rôle déterminant dans la progression de la rétinopathie diabétique, y
compris dans la forme œdémateuse.
•L’équilibre tensionnel diminue le risque de complications macro- et microangiopa-
thiques du patient diabétique.
•Le contrôle rigoureux de la pression artérielle retarde l’apparition et ralentit la pro-
gression de la rétinopathie diabétique.
•Lorsqu’un patient diabétique est porteur d’une rétinopathie, négliger le contrôle ten-
sionnel constitue une perte de chance.
•Il convient de rappeler le rôle majeur du contrôle glycémique dans la prévention et le
ralentissement de la progression de la rétinopathie diabétique chez les diabétiques,
et le caractère synergique puissant d’un contrôle tensionnel.
Les points essentiels

224 Pour la pratique
Médecine des maladies Métaboliques - Juin 2012 - Vol. 6 - N°3
Pour la pratique
224
[21] ACCORD Study Group; ACCORD Eye Study
Group, Chew EY, Ambrosius WT, Davis MD, et
al. Effects of medical therapies on retinopathy
progression in type 2 diabetes. N Engl J Med
2010;363:233-44[Erratum in: N Engl J Med
2011;364:190].
[22] Schrier RW, Estacio RO, Esler A, Mehler P.
Effects of aggressive blood pressure control in
normotensive type 2 diabetic patients on albu-
minuria, retinopathy and strokes. Kidney Int
2002;61:1086-97.
[23] Varma R, Macias GL, Torres M, et al.; Los
Angeles Latino Eye Study Group. Biologic risk
factors associated with diabetic retinopathy: the
Los Angeles Latino Eye Study. Ophthalmology
2007;114:1332-40.
[24] Klein R, Klein BE, Moss SE, Cruickshanks KJ.
The Wisconsin Epidemiologic Study of Diabetic
Retinopathy: XVII. The 14-year incidence and pro-
gression of diabetic retinopathy and associated
risk factors in type 1 diabetes. Ophthalmology
1998;105:1801-15.
[25] Bonnet S, Maréchal G. Influence de l’hyper-
tension artérielle sur la rétinopathie diabétique. J
Mal Vasc 1992;17:308-10.
[26] Ebrahimian TG, Tamarat R, Clergue M, et al.
Dual effect of angiotensin-converting enzyme
inhibition on angiogenesis in type 1 diabetic mice.
Arterioscler Thromb Vasc Biol 2005;25:65-70.
[27] Gilbert RE, Kelly DJ, Cox AJ, et al. Angiotensin
converting enzyme inhibition reduces retinal over–
expression of vascular endothelial growth factor
and hyperpermeability in experimental diabetes.
Diabetologia 2000;43:1360-7.
[28] Nagisa Y, Shintani A, Nakagawa S. The angio-
tensin II receptor antagonist candesartan cilexetil
(TCV-116) ameliorates retinal disorders in rats.
Diabetologia 2001;43:883-8.
[29] Chaturvedi N, Porta M, Klein R, et al.; DIRECT
Programme Study Group. Effect of candesartan
on prevention (DIRECT-Prevent 1) and progres-
sion (DIRECT-Protect 1) of retinopathy in type 1
diabetes: randomised, placebo-controlled trials.
Lancet 2008;372:1394-402.
[30] Chatuverdi N, Sjølie AK, Stephenson JM,
et al.; EUCLID Study Group. Effect of lisinopril
on progression of retinopathy in normoten-
sive people with type 1 diabetes. EURODIAB
Controlled Trial of Lisinopril in Insulin-Dependent
Diabetes Mellitus. Lancet 1998;351:28-31.
[31] UK Prospective Diabetes Study Group.
Efficacy of atenolol and captopril in reducing
risk of macrovascular and microvascular com-
plications in type 2 diabetes: UKPDS 39. BMJ
1998;317:713-20.
[32] Cusick M, Meleth AD, Agrón E, et al.;
Early Treatment Diabetic Retinopathy Study
Research Group. Associations of mortality and
diabetes complications in patients with type 1
and type 2 diabetes: early treatment diabetic
retinopathy study report no. 27. Diabetes Care
2005;28:617-25.
[33] Klein R, Klein BE, Moss SE, Cruickshanks KJ.
The Wisconsin Epidemiologic Study of Diabetic
Retinopathy. XV. The long-term incidence of
macular edema. Ophthalmology 1995;102:7-16.
et Recommandations). Diabetes Metab
2007;33(Suppl.1):1S1-1S105. www.has-sante.fr
[11] Laboureau-Soares Barbosa S, RodienP,
Draunet-Busson C, et al. Hypertension
artérielle chez le sujet diabétique. EMC-
Cardiologie;2011:11-301-P-10.
[12] UK Prospective Diabetes Study. Tight blood
pressure control and risk of macrovascular and
microvascular complications in type 2 diabetes:
UKPDS 38. BMJ 1998;317:703-13[Erratum in:
BMJ 1999;318:29].
[13] Dupas B, Massin P. Diagnostic et trai-
tement de la rétinopathie diabétique. EMC
Endocrinologie-Nutrition;2011:10-366-K-10.
[14] Kirkendall WM. Retinal changes of hyperten-
sion. In: Mausolf FA, editor. The eye and systemic
disease. Saint-Louis: Mosby, 1975:212-22.
[15] Klein R, Klein BE, Moss SE. The relation of
systemic hypertension to changes in the retinal
vasculature: the Beaver Dam Eye Study. Trans
Am Ophthalmol Soc 1997;95:329-48 ; discus-
sion:348-50.
[16] Wong TY, Mitchell P. Hypertensive retinopa-
thy. N Engl J Med 2004;351:2310-7.
[17] Knowler WC, Bennett PH, Ballintine EJ.
Increased incidence of retinopathy in diabe-
tics with elevated blood pressure. A six-year
follow-up study in Pima Indians. N Engl J Med
1980;302:645-50.
[18] Teuscher A, Schnell H, Wilson PW. Incidence
of diabetic retinopathy and relationship to base-
line plasma glucose and blood pressure. Diabetes
Care 1988;11:246-51.
[19] Chahal P, Inglesby DV, Sleightholm M, Kohner
EM. Blood pressure and the progression of mild
background diabetic retinopathy. Hypertension
1985;7:1179-83.
[20] Gaede P, Vedel P, Larsen N, et al.
Multifactorial intervention and cardiovascular
disease in patients with type 2 diabetes. N Engl
J Med 2003;348:383-93.
[3] Vu HT, Keefe JE, McCarty CA, Taylor HR.
Impact of unilateral and bilateral vision loss on
quality of life. Br J Ophthalmol 2005;89:360-3.
[4] Diabetes Control and Complications Trial
Research Group. The effect of intensive treatment
of diabetes on the development and progression
of long-term complications in insulin-dependant
diabetes mellitus. N Engl J Med 1993;329:977-86.
[5] Epidemiology of Diabetes Interventions and
Complications (EDIC). Design, implementation,
and preliminary results of a long-term follow-up
of the Diabetes Control and Complications Trial
cohort. Diabetes Care 1999;22:99-111.
[6] UK Prospective Diabetes Study (UKPDS)
Group. Intensive blood-glucose control with sul-
phonylureas or insulin compared with conven-
tional treatment and risk of complications in
patients with type 2 diabetes (UKPDS 33).
Lancet 1998;352:837-53[Erratum in: Lancet
1999;354:602].
[7] Ohkubo Y, Kishikawa H, Araki E, et al. Intensive
insulin therapy prevents the progression of dia-
betic microvascular complications in Japanese
patients with non-insulin-dependant diabetes
mellitus: a randomized prospective 6-year study.
Diabetes Res Clin Pract 1995;28:103-17.
[8] The World Health Organisation Multinational
Study of Vascular Disease in Diabetics. Diabetes
Drafting Group. Prevalence of small vessel and
large vessel disease in diabetic patients from 14
centres. Diabetologia 1985;28(Suppl.):615-40.
[9] Stamler J, Vaccaro O, Neaton JD, Wentworth D.
Diabetes, other risk factors, and 12-yr cardiovas-
cular mortality for men screened in the Multiple
Risk Factor Intervention Trial. Diabetes Care
1993;16:434-44.
[10] Agence française de sécurité sanitaire
des produits de santé-Haute Autorité de santé
(Afssaps-HAS). Recommandation profession-
nelle. Traitement médicamenteux du diabète
de type 2 (Actualisation). Novembre 2006.
Recommandation de bonne pratique (Synthèse
Le traitement de la rétinopathie diabétique menaçant la vue reste le traitement par
photocoagulation laser des cellules rétiniennes. Cependant, retarder la nécessité de
ce traitement protège le pronostic visuel. L’on comprend donc tout l’enjeu de ralentir
la progression de la RD.
Au vu des différentes études, il semble exister un lien entre HTA et progression de la
RD, ainsi qu’avec la progression de la maculopathie. Ainsi, l’équilibre tensionnel strict
(PA systolique ≤130mm Hg et PA diastolique ≤80mm Hg) participe au contrôle de la
progression de la RD.
Cependant, il n’existe pas de preuve suffisante justifiant d’introduire un traitement
antihypertenseur agissant sur le système rénine-angiotensine chez le diabétique nor-
motendu dans le but de ralentir, ou de prévenir, la RD.
Enfin, et surtout, il convient de rappeler le rôle majeur du contrôle glycémique dans la
prévention et le ralentissement de la progression de la RD chez les patients diabétiques,
ainsi que le caractère synergique puissant d’un contrôle tensionnel, comme cela fut
parfaitement démontré dans l’étude UKPDS chez les patients DT2.
Conclusion
1
/
5
100%