Copie de 20 11explan..

EXPLANTATION MATERIEL
DE STIMULATION
Défibrillateur - Pace Maker
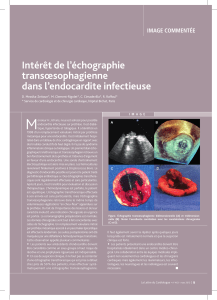
de l’infection locale à l’endocardite
Florence L’HOSTIS - Martine FIX - CHRU LILLE
AREPAC 2010 DOUAI

INTRODUCTION
•CHRU de LILLE: Centre important
pour les implantations de DAI, PM dont
une majorité de multi sites
•Patients avec pathologies lourdes =
terrain fragile

Introduction
•Centre de référence pour explantation :
Centres Hospitaliers + Cliniques
Nord - Pas de Calais , Picardie et Normandie
•Grand bassin de population
•Nombreux centres d’implantation
•Indications d’implantation plus étendues

Introduction
•CHRU Lille = Centre expérimenté
•Personnel médical + paramédical formés
•Techniques diversifiées (lasso de Cook,
laser, Spectranétics)
•Bloc dans l’enceinte bloc CCV

Indications et Recommandations
•Matériel endommagé:
-Chocs inappropriés
-Défaut de stimulation
-Elévation d’impédance
•Changement ou rajout
de sonde sur patient avec
thrombose veineuse
(upgrading de PM en
DAI)
Patient non infecté
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
1
/
29
100%