Atteinte urétérale après chirurgie du carrefour aortique

ARTICLE ORIGINAL Progrès en Urologie (2000), 10, 1156-1160
1156
Atteinte urétérale après chirurgie du carrefour aortique.
A propos de 6 cas
Luc CLEMENS, Stéphane BERNARDINI, Eric CHABANNES, François DEBIERE, Hugues BITTARD
Service d’Urologie, CHR Saint-Jacques, Besançon, France
La chirurgie vasculaire est la 3ème cause de lésions
urétérales après la chirurgie gynécologique et la chirur-
gie digestive, avec moins de 1,75% d’atteinte urétérale
de toute la chirurgie pelvienne [3]. Ces lésions évoluent
en trois stades après chirurgie vasculaire : aigu, subai-
gu et chronique. Seuls 30% des traumatismes urétéraux
sont reconnus durant l’intervention, la majorité des cas
évoluant sur un mode chronique [30].
Le but de ce travail à travers 6 observations a été d’étu-
dier ces complications urétérales et les différentes pos-
sibilités thérapeutiques pouvant être appliquées.
MATERIEL ET METHODE
Notre étude s’intéressait aux possibilités thérapeu-
tiques en fonction du délai d’apparition de la sténose
urétérale et de la chirurgie vasculaire, de sa longueur, et
de l’état général du patient. 6 patients ont été pris en
charge entre 1990 et 1998. La moyenne d’âge était de
64,6 ans ± 8,21 (extrêmes : 52 ans-75 ans). On notait
dans les antécédents vasculaires 3 prothèses du carre-
four aortique, un pontage iliaque et un patch iliaque
d’agrandissement. Le matériel utilisé était du Dacron,
dans tous les cas.
Dans un cas, il s’agissait d’une péri-urétérite au stade
subaigu. Pour les 5 autres patients, il s’agissait d’une
évolution chronique. Le délai écoulé avant le diagnos-
tic était de 11,6 ans ± 4,04.
Une urographie intraveineuse (UIV) était réalisée dans
tous les cas, le scanner abdominal (TDM) pour 4 cas,
une urétéropyélographie rétrograde (UPR) pour 2 cas
et une scintigraphie rénale pour 4 cas. La scintigraphie
était demandée en cas d’insuffisance rénale avant la
prise en charge urologique (n=3) et pour un cas, après
1 an de corticoïdes (patient n°4).
Manuscrit reçu : janvier 2000, accepté : juin 2000.
Adresse pour correspondance : Dr. L.Clemens, Service d’Urologie, CHR Saint-
Jacques, 2, place Saint-Jacques, 25030 Besançon Cedex.
RESUME
But : Le but de cette étude est d’évaluer la prise en charge et les possibilités théra-
peutiques actuelles des complications urétérales après chirurgie vasculaire;
Patients et Méthode : 6 patients ont été pris en charge entre 1990 et 1998 (âge
moyen: 64,7 ans) pour complication urétérale après chirurgie du carrefour aor-
tique. Le délai moyen entre la chirurgie vasculaire et la prise en charge uro l o g i q u e
était de 11,6 ans (± 4,04). Tous les patients ont eu une urographie intraveineuse
(UIV), et 4 patients une tomodensitométrie (TDM) abdominale. Ces complications
étaient : 2 sténoses urétérales, 1 péri-urétérite inflammatoire, 2 péri-urétérites
c h roniques et une compression par un pseudo-anévrisme. Le siège était iliaque
dans tous les cas.
Résultats : le traitement a été une pose de sonde JJ provisoire (n=1), une urétérolyse
(n=1), une endo-dilatation (n=1), une reconstruction par vessie psoïque (n=1) et une
corticothérapie (n=2). Il y a eu 4 succès, un échec (corticothérapie), et un décès pour
une autre cause.
Conclusion : L’atteinte urétérale après chirurgie vasculaire est une affection rare de
découverte souvent fortuite. L’atteinte iliaque est prédominante. L’UIV et la TDM
sont les examens paracliniques de référence. Les possibilités thérapeutiques dépen-
dent en premier lieu de l’état général du patient.
Mots clés : Sténose urétérale, chirurgie vasculaire, complications, traitement.

1157
Le succès thérapeutique a été défini sur plusieurs cri-
tères : évolution clinique, disparition de la sténose et de
la dilatation sus-jacente.
RESULTATS
Les résultats sont résumés dans le Tableau 1.
Les coliques néphrétiques étaient révélatrices pour 4
cas, une septicémie à E. coli pour un cas et une décou-
verte fortuite dans le cadre d’un bilan de suivi d’un
EOA buccal. L’examen clinique en dehors de la patho-
logie révélatrice était sans particularité.
L’UIV mettait en évidence l’obstacle dans tous les cas.
L’UPR était réalisée quand existait un doute sur sa lon-
gueur. L’aspect radiographique sténotique était com-
mun aux sténoses, aux péri-urétérites (subaiguës ou
chroniques) et aux compressions extrinsèques.
L’obstacle était iliaque court pour 4 cas et ilio-pelvien,
supérieur à 2 cm pour les 2 autres. Le scanner abdomi-
nal était demandé pour étudier la position de l’uretère
par rapport à la prothèse et/ou pour bilan étiologique. Il
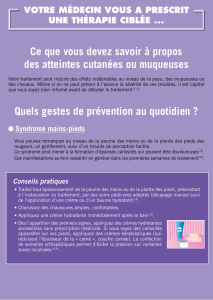
s’agissait d’une sténose pure (n=2), d’une péri-urétéri-
te inflammatoire subaiguë (n=1), d’une péri-urétérite
chronique ou fibrose engaînante (n=2) et d’une com-
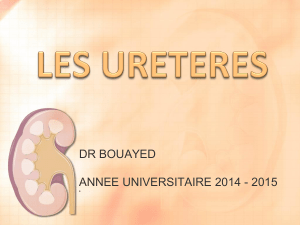
pression par un pseudo anévrisme (n=1) (Figure 1).
Le traitement était médical par corticoïdes (n=2), endo-
scopique (n=2) et chirurgical (n=2).
Le traitement endoscopique a consisté en une dériva-
tion provisoire par sonde JJ et une dilatation endosco-
pique par ballonnet à haute pression. Le traitement chi-
rurgical a été réalisé pour fibrose engaînante longue de
l’uretère (n=2). Il consistait en une urétérolyse et une
vessie psoïque. Les résultats de la corticothérapie se
sont soldés par le décès d’un patient après un mois de
prescription (évolution carcinologique de l’EOA buc-
cal) et un échec.
Au total , sur 6 patients, nous notons 4 succès, un échec
et une évolution inconnue par le décès du patient d’une
autre cause qu’urologique. Nous n’avons noté aucune
altération de la fonction rénale après chirurgie. Le recul
total était de 2,18 ans.
DISCUSSION
Les complications urétérales secondaires à la chirurgie
vasculaire sont rares (0,5% à 5%) [26, 27, 29, 30].
Seulement 6 patients en ont présenté depuis la pose de
prothèse vasculaire dans notre centre hospitalier. Toute
découverte de lésion urétérale doit être prise en comp-
L.Clemens et coll., Progrès en Urologie (2000), 10, 1156-1160
Tableau 1. Patients présentant une complication urétérale après chirurgie du carrefour aortique. Données cliniques.
Patients Age Chirurgie Atteinte Intervalle Lésion Clinique Localisation Traitement Recul Résultat
(ans) vasculaireurétérale (évolution)
N° 1 75 1983 1995 12 ans Compression Coliques Ilio- Urétérolyse 1 an Succès
Patch (chronique) par pseudo- néphrétiques pelvienne
anévrisme
N° 263 1988 1995 7 ans Sténose Coliques Iliaque Endo- 2 ans Succès
prothèse aorto- (chronique) néphrétiques dilatation
bifémorale
Dacron®
N° 3 65 1985 1996 11 ans Sténose Découverte Iliaque Corticoïdes 1 mois DCD
prothèse (chronique) fortuite autre cause
aorto-
bifémorale
Dacron®
N° 452 1985 1995 10 ans Péri-urétérite Coliques Iliaque Corticoïdes 1 an Echec
prothèse aorto- (chronique) (fibrose néphrétiques Perdu
bifémorale engainante) de vue
Dacron®
N° 5 72 1990 1990 1 mois Péri-urétérite Septicémie Iliaque JJ provisoire 8 ans Succès
Prothèse (sub-aigu) inflammatoire à E. Coli
aortique
Dacron®
N° 6 61 1980 1998 18 ans Péri-urétérite Coliques Ilio- Vessie psoïque 1 an Succès
Pontage iliaque (chronique) (fibrose néphrétiques pelvienne
Dacron® engainante)

te car l’incidence de la néphrectomie est de 32% en cas
de diagnostic tardif contre 4,5% dans les cas précoce-
ment dépistés [3, 14)] L’âge moyen de notre groupe
correspond à celui d’une population vasculaire [10,
21].
On distingue 3 types de lésions dans le temps qui
entraînent des traitements différents : les atteintes
aiguës, subaiguës et chroniques.
Les lésions aiguës apparaissent dans le mois post-opé-
ratoire. Il s’agit des sections ou microtraumatismes. La
plupart sont méconnues pour 30% des cas et évoluent
sur le mode chronique. La résection/suture est le traite-
ment le plus adapté [3, 34] Le risque de blessure peut
être diminué par la mise en place de sondes urétérales
en préopératoire dans les cas difficiles [30]. Pour
BENNANI et ROBERT, ce cathétérisme augmenterait la
rigidité urétérale et les risques de traumatisme par
l’opérateur [3, 29]. L’alternative est proposée par FRY
avec une injection de bleu indigo carmin en per-opéra-
toire [14].
Les lésions subaiguës sont des péri-urétérites secon-
daires à une inflammation rétropéritonéale et urétérale.
Elles apparaissent après le mois post-opératoire.
L’abstention thérapeutique est la règle, les lésions dis-
paraissant dans l’année [5, 16, 30]. Seules les compli-
cations infectieuses, comme a présenté le patient n°5,
ou algique doivent être traitées par une dérivation pro-
visoire.
Les lésions chroniques se développent après la premiè-
re année. Il s’agit de sténose, de péri-urétérite par fibro-
se engaînante ou de compression par un corps extrin-
sèque (bras de prothèse, pseudo-anévrisme). Au stade
chronique, les fibroses engaînantes et sténoses ont la
même prise en charge qui dépendra de la longueur de
l’obstacle, de l’état fonctionnel du rein sus-jacent et de
l’état général du patient. Pour faciliter la compréhen-
sion de ce travail, le mot sténose désignera ces 2 états.
Le délai avant le diagnostic des lésions chroniques
dans notre série est de 11 ans en moyenne. Elles sont
souvent sous-estimées car asymptomatiques, avec une
évolution de 10 à 15 ans après intervention vasculaire
[21, 30)] La découverte est souvent fortuite et justifie-
rait d’une surveillance à vie pour ces patients [21, 30].
Quand elle existe, la symptomatologie clinique est
variée. La colique néphrétique en est le signe révéla-
teur le plus fréquent (n=4) [27]. Il semblerait que le
Dacron® soit un facteur péjoratif supplémentaire par la
fibrose réactionnelle à son contact [18, 25, 30].
L’échographie est un examen incontournable objecti-
vant l’urétéro-hydronéphrose, permettant un suivi peu
agressif. L’UIV (n=6) et la TDM abdominale (n=4)
sont essentielles au diagnostic. L’UIV objective dans
90% des cas l’obstacle urétéral [3, 5, 13]. La TDM pré-
cise son siège et sa nature [8, 13]. Elle peut étudier la
position de la prothèse vasculaire par rapport à l’uretè-
re, et toute autre cause d’obstruction extrinsèque [30].
L’UPR (n=2) situe l’obstacle, son niveau, sa longueur
et l’état de l’uretère en aval de la lésion en complément
de l’UIV [3, 10, 14]. L’atteinte iliaque est particulière à
la chirurgie vasculaire [3, 29]. Ces examens morpholo-
giques permettent l’évaluation approximative de la
valeur fonctionnelle rénale [22, 24]. Ils seront proba-
blement dépassés par l’angio-IRM couplée à l’uro-
IRM (URM) qui ne nécessite ni irradiation ni d’injec-
tion de produit de contraste [28]. Des coupes en recons-
truction 2D et 3D, plus performantes, permettent en
séquence T1 l’analyse du carrefour aortique et de ses
branches. La sensibilité est supérieure ou au moins
égale à l’artériographie [19, 28]. Le même examen en
séquence T2 étudie le tractus urinaire, détecte l’obs-
truction, analyse l’uretère et le milieu péri-urétéral
avec une sensibilité de 88% à 100% [7, 23]. Cet exa-
men est particulièrement utile pour les étiologies
inflammatoires péri-urétérales [17]. L’IRM permettrait
d’évaluer dans le même temps la fonction rénale [32].
Les corticoïdes représentent le traitement médical
(n=2). Si FELDBERG les défend en alternative à la chi-
rurgie, la plupart des auteurs les rejettent face aux
risques de fistules secondaires ou de sepsis grave et
leur inefficacité au stade chronique [5, 12, 16, 30]. Au
vu de la littérature et de notre série, nous pensons que
la corticothérapie demeure utile dans 2 cas : en préopé-
ratoire afin de réduire la gangue inflammatoire péri-
urétérale, et en période subaiguë. Elle est alors surtout
efficace au premier semestre et pourraient prévenir les
risques de fibroses secondaires [5, 12, 16]. Leur
1158
Figure 1. Volumineux pseudo-anévrisme révélé par une crise
de colique néphrétique. L’uretère roule en avant sur la masse
anévrismale : urétérolyse et cure du pseudo-anévrisme dans le
même temps opératoire.
L.Clemens et coll., Progrès en Urologie (2000), 10, 1156-1160

meilleure place nous semble être une aide à la prépara-
tion de l’intervention comme HUBEN le préconise [16].
Nous n’avons pas choisi le drainage à demeure par
sonde JJ devant les risques de drainage à long terme [2,
11, 33]. L’indication de maintenir une sonde JJ en trai-
tement définitif doit être posée devant l’impossibilité
d’appliquer d’autres moyens thérapeutiques [29, 33].
Le meilleur traitement des sténoses courtes en première
intention est la dilatation au ballonnet à haute pression.
Elle est indiquée pour les sténoses inférieures à 2 cm
(n=1). Cette technique cumule les avantages d’un coût
d’utilisation modéré, une courte durée d’hospitalisation,
une faible morbidité ne gênant pas une chirurgie de rat-
trapage [26]. Il n’y a pas de limite dans le nombre de
séances [9]. Il semblerait que le paramètre le plus prédic-
tif de succès soit la longueur de l’obstacle. Le succès est
estimé à 100% à 5 ans par F
L A M
si il est inférieur à 1,5
cm [13]. L’importance du rétrécissement est le second
critère de succès [33, 34]. Les autres facteurs sont l’ab-
sence de péri-urétérite et sa découverte récente depuis la
c h i r u r gie vasculaire [3, 20, 26, 27]. Les échecs survien-
nent pour 80% des cas dans les 3 premiers mois [18]. Le
taux de succès à long terme diminue avec le recul. N
E T TO
publie un taux de succès stable de 57% avec un recul
moyen de 2 ans [26]. La récidive précoce est prédictive
d’échec d’une nouvelle tentative [26, 27]. La dilatation
peut être suivie d’une urétérotomie interne à lame froide
ou thermique en dehors des zones au contact de prothèse
vasculaire ou digestive [35]. Y
A M A D A
obtient des résul-
tats satisfaisants avec 85% de succès avec un recul de 18
mois [35]. En cas d’échec, la chirurgie demeure la réfé-
rence [13, 20, 27]. L’alternative est la résection/anasto-
mose avec des résultats oscillants de 50% à 70% de suc-
cès à long terme [3, 14, 27].
L’exérèse/réimplantation est proposée pour l’atteinte
distale de l’uretère au niveau de la jonction urétéro-
vésicale [3].
La réimplantation sur vessie psoïque est indiquée pour
les atteintes distales et longues de l’uretère ilio-pelvien
(n=1). Nous préférons cette technique au lambeau de
Boari devant sa facilité de réalisation et le peu de com-
plication (moins de 10% de complications contre 30%)
[4, 20]. La technique de réimplantation n’est pas impor-
tante. Pour WITTERS, seule compte la création d’un tra-
jet sous muqueux d’au moins 2 cm [34].
L’urétérolyse (n=1) est peu utilisée devant le risque
important de dévascularisation sur un uretère fragilisé
par une chirurgie antérieure, les risques d’une dissec-
tion difficile et hasardeuse [8, 18].
L’iléo-urétéroplastie est une intervention peu proposée
malgré de bons résultats. Une meilleure codification de
la technique permettrait d’élargir son emploi [1, 4, 15,
20, 25]. L’autogreffe serait préférable pour une atteinte
urétérale basse à une plastie vésicale difficile tout en
respectant l’intégrité fonctionnelle urinaire [4, 6, 25].
Dans certains cas, une des branches de la prothèse vas-
culaire peut être placée en avant de l’uretère, réalisant
une pince constrictive [5, 18]. La tactique opératoire
est question d’école. L’intervention consiste soit en une
reconstruction urétérale, soit vasculaire. Pour
CUSSENOT, SCHEIN et WALJIN, la prothèse doit être sec-
tionnée et placée en arrière de l’uretère en raison des
risques infectieux, toujours possible dans un geste uri-
naire [24, 30, 31]. Pour BLASCO et KAUFMANN, le trai-
tement est une résection/anastomose de l’uretère avec
intrapéritonisation [9, 18]. Ce choix repose sur le
risque septique et thrombotique de la prothèse par les
manipulations chirurgicales, avec un contrôle et un
clampage malaisés.
CONCLUSION
Les complications urétérales après chirurgie vasculaire
sont une affection rare, de découverte souvent fortuite.
Les formes chroniques asymptomatiques sont les plus
fréquentes. Le bilan lésionnel comprend une UIV et
une TDM abdominale et bientôt l’angio-IRM couplée à
l’uro-IRM (URM). L’atteinte iliaque courte est la plus
fréquente et doit être traitée, ou au moins suivie. Nous
pensons que le traitement est chirurgical. Il repose en
premier sur une endo-dilatation, peu agressive, qui
n’empêche pas une chirurgie en cas d’échec dans un
2ème temps. L’exérèse/anastomose est la chirurgie des
obstacles courts, la vessie psoïque, celle des obstacles
longs. L’iléoplastie demeure exceptionnelle.
L’utilisation de la sonde JJ à demeure doit se faire chez
une population sélectionnée. Par notre expérience,
nous réservons les corticoïdes à des cas biens définis
et uniquement en vue d’une intervention. Souvent
l’état général du patient limite les possibilités théra-
peutiques.
REFERENCES
1. ABOUTAIEB R., EL MOUSSAMI A., BENNANI S., MRINI M.,
BENJELLOUN S. Les urétéro-plasties. J. Urol. (Paris), 1996, 102,
57-59.
2. AWAKURA Y., YAMAMOTO M., OKUNO H., HASHIMURA T.,
FUKUYAMA T., OTANI T. et al. A case of uretero-aortic fistula
Hinyokika of urology 1997, 43, 299-301.
3. BENNANI S., ABOUTAIEB R., EL MRINI M., BENJELLOUN S.
Les traumatismes de l’uretère à propos de 29 cas. J. Urol. (Paris),
1994, 239-247.
4. BENSON M.C., RING K.S., OLSSON C.A. Ureteral reconstruction
and bypass : experience with ileal interposition, the Boari flap hitch
and renal autotransplatation. J. Urol., 1990, 143, 20-23.
5. BLASCO F.J., SALADIE J.M. Ureteral obstruction and ureteral fis-
tulas after aortofemoral or aortoiliac Bypass surgery. J. Urol., 1991,
145, 237-242.
6. BODIE B., NOVICK A., ROSE M. Long terme results with renal
autotransplantation for ureteral replacement. J. Urol. 1986, 136,
1187-1189.
1159
L.Clemens et coll., Progrès en Urologie (2000), 10, 1156-1160

7. CATALANO C., PAVONE P., LAGHI A., SCIPIONI A., PANE-
BIANCO V., BRILLO R., FRAIOLI F., PASSARIELLO R. MR
pyelography and conventional MR imaging in urany tract obstruc-
tion. Acta Radiol., 1999, 40, 192-202.
8. CORMIER J.M. Fibrose rétropéritonéale , péri-anévrismale aortite
inflammatoire avec insuffisance rénale : 4 observations. Quel traite-
ment? Technique et stratégie en chirurgie vasculaire. Paris, AERCV,
1990, 129-136.
9. DE LA TAILLE A., RAVERY V., HOFFMANN P., HERMIEU J.F.,
MULINIER F., DELMAS V., BOCCON-GIBOD L. Le traitement
des sténoses de l’uretère par cathéter de dilatation à haute pression.
Prog. Urol., 1997, 7, 408-414.
10. DOWLIN G.R., CORRIERE J., SANDLER C. Iatrogenic ureteral
injury. J. Urol., 1986, 135, 912-915.
11. EL KHADER K., KOUTANI A., TAZI K., IBEN ATTYA A.,
HACHIMI M., LAKRISSA A. Drainage interne par sonde double J.
A propos de 91 cas. Ann. Urol., 1996, 30, 235-239.
12. FELBERG M., HENE R. Perineurysmal fibrosis and its response to
corticosteroïd treatment : a computerized tomography followup in a
case. J. Urol., 1983, 130, 1163-1164.
13. FLAM T., MARTIN X. Traitement endo-urologique des sténoses de
l’uretère et de la jonction pyelo-urétérale. Prog. Urol., 1, 771-864.
14. FRY D.E., MINHOLEN L., HARBRECHT P.J. Iatrogenic uretera
injury. Option in management. Arch Surg., 1983, 118, 454-457.
15. GOSALBEZ R., GOUSSE E. Reconstruction after undiversion of
the short or severely dilated ureter : the anti-reflux ileal nipple revi-
sited. J. Urol., 1998, 159, 530-534.
16. HUBEN R.P., SCHELLHAMMER P.F. Steroid therapy for ureteral
obstruction after aortoiliac graft surgery. J. Urol., 1981, 125, 881-
883.
17. HUSSEIN S., O’MALLEY M., JARA H., SADEGHI-NEJAD H.,
YUCEL E.K. MR urography. Magn. Reson. Imaging Clin. N. Am.
1997, 5, 95-106.
18. KAUFMANN J.E., LOWELL PARSONS C., GOSINK B.B.
Retrospective study of ureteral obstruction following vascular
bypass surgery. Urology, 1982, 19, 278-283.
19. KELKIS M.L., SEMELKA R.C., WORAWAT TANAKUL S.,
MOLINA P.L., MAURO M.A. Magnetic resonance imaging of the
abdominal aorta and iliac vessels using combined 3-D gadolinium-
enhanced MRA and gadolinium-enhanced fat-suppressed spoiled
gradient echo sequences. Magn. Reson. Imaging, 1999, 17, 641-651.
20. KOUTANI A., LECHEVALLIER E., BRETHEAU D., COULAN-
GE C. Traitement chirurgical des sténoses iatrogène de l’uretère. J
Urol. (Paris), 1996, 102, 145-149.
21. LITOOY F.N., STEFFAN G., STEIMANN S., SALETTA C.,
GREISLER H.P. An 11 year experience with aortofemoral bypass
grafting. Cardiovasc. Surg., 1993, 1, 232-238.
22. LOTTI T., D’ARMIENTO M., ZITOI A., DE SIO M. Les actuelles
techniques diagnostiques dans la prédiction de la reprise fonction-
nelle d’un rein urographiquement exclu. J. Urol. (Paris), 1986, 91-
95.
23. LOUCA G., LIBEROPOULOS K., FIDAS A., NIKOLAPOULOU,
LYKOURINAS M., STRIGARIS K. MR urography in the diagno-
sis of urinary obstruction. Eur. Urol., 1999, 35, 102-108.
24. MANGIN P., PASCAL B., RICHARD F. Valeur des examens isoto-
piques dans l’appréciation de la fonction et la récupération d’un rein
en obstruction. Chirurgie, 1987, 113, 270-276.
25. MARTIN X., NDOYE A., KONAN P.G., FEITOSA TAJRA L.C.,
GELET A., DAWAHRA M. Des dangers de l’urétéroscopie à l’éta-
ge lombaire : à propos de 4 cas d’avulsion de l’uretère. Prog. Urol.,
1998, 8, 358-362.
26. NETTO J.R., FERREIRA U., LEMOS S.G., CLARO JF.
Endourological management of ureteral strictures. J. Urol., 1990,
144 , 631-634.
27. O’BRIEN W.M., MAXTED W.C., PAHIRA J.J. Ureteral stricture :
experience with 31 cases. J. Urol., 1988, 140, 737-740.
28. PEETRONS P. Perspectives futures de l’imagerie médicale. Rev.
Med. Brux., 1999, 20, 362-364.
29. ROBERT M., DRIANNO N. Traumatisme urétéraux au cours de la
chirurgie des anévrismes de l’aorte abdominale sous rénale. J. Chir.,
1995, 132, 127-130.
30. SCHEIN M., SAADIA R. Ureteral obstruction after abdominal aor-
tic surgery. Am. J. Surg., 1991, 162, 86-89.
31. WALJIN E., RENDERS G., VEREECKEN L. Urological complica-
tions folloming aortofemoral bypass graft. Br. J. Urol., 1975, 47,
617-621.
32. WEN J.G., CHEN Y., RINGGAARD S., FROKIAER J., JORGEN-
SEN T.M., STODKILDE-JORGASEN H., DJURRUS J.C.
Evaluation of renal function in normal and hydronephrotic kidneys
in rats using gadoloinium diethylenetetramine-pntaacetic acid
enhanced dynamic magnetic resonance imaging. J. Urol., 2000, 16,
1264-1270.
33. WITJES JA. Breakage of silicone double pigtail stent as a long terme
complication. J. Urol., 1993, 150, 1898-1899.
34. WITTERS S., CORNELISSEN M., VEREECKEN R. Iatrogenic
ureteral injury : agressive or conservative treatment. Am. J. Obstet.
Gynecol., 1986, 155, 582-584
35. YAMADA O., ONO Y., OSHIMA S., MIYAKE K. Transurethral
ureteroscopic ureterotomy assisted by a prior ballon dilatation for
releving ureteral stricture. J. Urol., 1995, 153, 1418-1421.
____________________
SUMMARY
Ureteric lesions after surgery of the aortic bifurcation.
Report of 6 cases.
Objective: The objective of this study was to evaluate the mana -
gement and current treatment options for ureteric complications
after vascular surgery based on a series of 6 cases.
Patients and Method::6 patients were treated between 1990 and
1998 (mean age: 64.7 years) for ureteric complications after
aortic bifurcation surgery. The mean interval between vascular
surgery and urological management was 1
1.6 years (± 4.04). All
patients were assessed by intravenous urography (IVU), and 4
patients were assessed by abdominal computed tomography
(CT). These complications consisted of: 2 cases of ureteric ste -
nosis, 1 case of inflammatory peri-ureteritis, 2 cases of chronic
peri-ureteritis and 1 case of compression by a false aneurysm.
The lesion was situated in the iliac ureter in every case.
Results: Treatment consisted of temporary double J stenting
(n=1), ureter release (n=1), endoscopic dilatation (n=1), psoas
bladder reconstruction (n=1) and corticosteroid therapy (n=2),
with 4 successes, 1 failure (corticosteroid therapy), and 1 death
from another cause.
Conclusion: Ureteric lesion after vascular surgery is a rare
complication, often discovered incidentally. The iliac ureter is
predominantly affected. IVU and CT are the reference examina -
tions. Treatment options primarily depend on the patient's gene -
ral state.
Key-words: Ureteric stenosis, vascular surgery, complications,
treatment.
1160
____________________
L.Clemens et coll., Progrès en Urologie (2000), 10, 1156-1160
1
/
5
100%