Lire l'article complet

Le Courrier des addictions (15) – n ° 2 – Avril-mai-juin-2013
21
Alcoholic liver disease, responsible for 10,000 deaths/year in France, is the first indication for liver
transplantation and represents 27% of all indications. Alcoholic disease is a systemic disease cau-
sing extra hepatic damages, which require exploration before liver transplantation (LT). Less than
10% of the patients with an alcoholic cirrhosis are referred to a transplant center and only 3% of
them will benefit from a LT. Considering objective parameters such as rejection, infection and sur-
vival after LT, decompensated alcoholic cirrhosis is an excellent indication for LT with survival rates
at 1 and 5 years representing respectively 84% and 73%. Relapse after LT, which occurs in less than
25% of cases, should be screened and referred to a substance abuse specialist. The “6-months-
rule” must no longer be, and even acute alcoholic hepatitis could be a valuable indication for LT.
Mots-clés :
Maladie alcoolique
du foie, hépatite alcoolique aiguë,
transplantation hépatique,
règle des 6 mois, rechute
Keywords:
Alcoholic liver disease, acute
alcoolic hepatitis, liver transplantation,
the “6 months rule”, relapse
Transplantation hépatique
pour maladie alcoolique : question
scientifique ou question “morale” ?
Liver transplantation in alcoholic liver disease:
ethical or scientific issue?
S. Faure*, G.P. Pageaux*
La cirrhose alcoolique, responsable d’environ 10 000 décès/an en France, est la pre-
mière cause de transplantation hépatique (TH), avec 27 % des indications de greffe. La
maladie alcoolique est “systémique”, avec des atteintes extrahépatiques qu’il convient
de rechercher lors de l’évaluation avant la greffe. Moins de 10 % des patients présentant
une cirrhose alcoolique décompensée sont adressés à un centre de transplantation et
seuls 3 % bénéficieront d’une TH. Selon des critères objectifs, tels que le rejet, le taux
d’infection et la survie après la greffe, la cirrhose alcoolique décompensée est une excel-
lente indication de TH, avec une survie à 1 et 5 ans de 84 % et 73 %, respectivement. La
reprise d’une consommation d’alcool après TH, qui survient dans moins de 25 % des cas,
doit être dépistée et prise en charge par une équipe spécialisée en addictologie. La “règle
des 6 mois” ne doit plus être une condition intangible à la TH, et même l’hépatite alcoo-
lique aiguë grave corticorésistante peut s’avérer être une indication pertinente de TH.
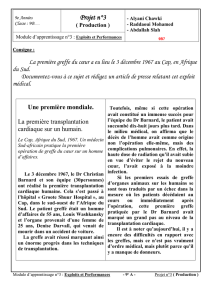
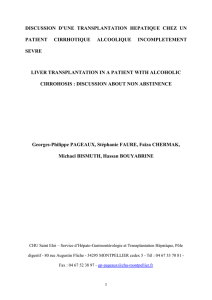
Alcoolique
16 284 – 33 %
Virale +
alcoolique
2 205 – 4 %
Auto-immune
2 019 – 4 %
Biliaire
secondaire
590 – 1 %
Biliaire
primitive
4 702 – 9 %
Autres
970 – 2 %
De causes
inconnues
3 793 – 8 %
Virale
19 646 – 39 %
Cirrhoses
Figure 1.
Répartition des scores DASH du module
général selon le statut professionnel de janvier
1998 à décembre 2012 en Europe.
* Service d’hépato-gastroentérologie et de transplantation
hépatique, hôpital Saint-Éloi, CHU de Montpellier.
Ces chiffres révèlent l’évolution des mentalités,
puisque la cirrhose alcoolique représentait seu-
lement 4,6 % des indications en 1983. Cette évo-
lution a été possible grâce aux résultats probants
de la TH dans cette indication. Pourtant, les
patients porteurs d’une cirrhose alcoolique sont
encore sous-référencés auprès des centres de
greffe et la durée d’abstinence nécessaire avant
la greffe reste débattue.
Quels sont les candidats
à une transplantation
hépatique pour cirrhose
alcoolique ?
Lors de la conférence, en 1983, des NIH
(National Institutes of Health), la cirrhose
alcoolique a été reconnue pour la première fois
comme une indication acceptable de TH chez
des patients abstinents et présentant des critères
cliniques péjoratifs. La survie à 5 ans chez les
patients atteints de cirrhose alcoolique décom-
pensée est inférieure à 20 % en l’absence de TH
et supérieure à 70 % s’ils sont transplantés.
En 1999, l’étude de T. Poynard et al. a montré
que la cirrhose alcoolique décompensée (Child-
PughC allant de 11 à 15) était une indication
justifiée de TH, avec un bénéfice en termes de
survie, alors qu’elle n’apportait aucun gain de
survie pour les patients Child-PughA(1). Une
étude prospective multicentrique française
pilotée par le centre de Besançon a suggéré que
la TH était délétère en cas de cirrhose du foie
compensée Child-Pugh B, avec une surmortalité
liée à l’augmentation du risque carcinologique
de novo (2).
Le score de MELD (Model for End-stage Liver
Disease) a remplacé depuis le score de Child-
Pugh, trop imprécis du fait de 2variables cli-
niques et subjectives. Le score de MELD a ini-
tialement été élaboré pour prédire la mortalité
à 3mois après pose de TIPS (Transjugular
Intrahepatic Portosystemic Shunt) chez des
patients cirrhotiques. Il se calcule à partir de
3variables biologiques : la bilirubine, la créati-
nine et l’International Normalised Ratio (INR)
selon la formule qui suit :
MELD= 3,78 × ln bilirubine (mg/dl) + 11,2 ×
ln INR + 9,57 × ln créatinine (mg/dl) + 6,43.
Il a ensuite été démontré que la mortalité sur
liste d’attente de TH était directement corrélée
au MELD (par exemple, pour les patients avec
MELD=40, la mortalité sur liste est 300fois
supérieure à celle des patients de MELD
compris entre 6et11)[3]. Le bénéfice de la
TH en termes de survie est évident au-delà
de18, mais chez les patients avec un score en
deçà de18, la mortalité est plus élevée en cas
de greffe(4). Cependant, une récente étude
rétrospective de la base de données UNOS
E
n France, 2millions de personnes sont
dépendantes de l’alcool et 6mil-
lions ont une consommation à
risque. La Haute Autorité de santé (HAS)
estime à 15 % le nombre de buveurs exces-
sifs d’alcool. L’alcool est la troisième cause
de décès prématurés et évitables après le
tabac et l’hypertension artérielle (HTA).
La cirrhose alcoolique est responsable de 9 000à
10 000 décès par an en France et représente la
première cause de mortalité imputable à l’alcool.
Elle est la première indication de transplanta-
tion hépatique (TH) en France et la deuxième
en Europe et aux États-Unis. Selon l’Agence
française de biomédecine, on dénombre, en
2011, 1 164 greffes hépatiques dont 27 % pour
maladie alcoolique du foie. Selon le Registre
européen de transplantation hépatique (Euro-
pean Liver Transplant Registry [ELTR]), sur la
période allant de 1988 à 2010, 33 % des greffes
pour cirrhose et 21 % des greffes toutes causes
confondues avaient pour indication principale
la cirrhose alcoolique (figure 1).

Le Courrier des addictions (15) – n ° 2 – Avril-mai-juin 2013 22
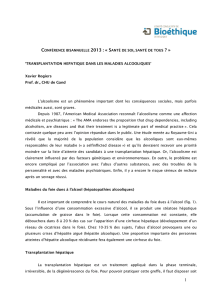
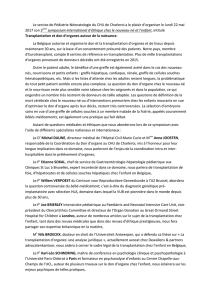
210
0
60
80
86
82
83 80
75 71
79
74
73
69 64
63
59
58
100
4
Années
Survie (%)
3 65 8
7109
Cirrhose virale : 19 574 Cirrhose alcoolique : 16 260 Cirrhose biliaire primitive : 4 697
p log-rank :
Cause virale versus alcoolique : 0,01
Cause virale versus cirrhose biliaire primitive : 0,0001
Cause alcoolique versus cirrhose biliaire primitive : 0,0001
Figure 2.
Survie des patients ayant pour première indication une cirrhose.
(United Network for Organ Sharing) a retrouvé
un bénéfice en termes de mortalité sur liste et
de survie post-transplantation chez des patients
avec cirrhose alcoolique “pure” ayant un score
de MELD plus bas (5).
Ainsi, le MELD est utilisé aux États-Unis depuis
2002 pour déterminer l’ordre d’attribution des
greffons selon la politique du “sickest first”. En
France, la règle d’attribution des greffons hépa-
tiques a changé en mars 2007, elle est désormais
fondée sur le score Foie, dont la principale com-
posante est le score MELD.
En donnant la priorité aux patients les plus
graves, l’égalité des chances pour l’obtention d’un
greffon a été optimisée, avec une réduction du
délai et, surtout, de la mortalité sur liste d’attente.
La TH est la meilleure option thérapeutique
chez les patients atteints de cirrhose alcoolique
décompensée.
Il existe cependant des contre-indications
générales à la TH : une atteinte viscérale
grave, un antécédent de cancer (datant de
moins de5ans) et, a fortiori, un cancer évo-
lutif (hormis un carcinome hépatocellulaire
[CHC]), et un âge physiologique avancé. Pour
cela, un bilan approfondi, prenant en compte le
terrain spécifique de ces patients, est nécessaire
avant la greffe.
Un bilan exhaustif
avant la greffe
Chez les patients ayant une cirrhose alcoo-
lique, l’intoxication alcoolique chronique peut
entraîner des atteintes organiques extrahépa-
tiques qui doivent être recherchées au cours
du bilan avant la greffe. L’inscription de ces
malades en liste d’attente nécessite, comme
spécifié par la conférence de consensus de 2005,
“un bilan prégreffe parti culièrement attentif
à la recherche des lésions liées à une toxicité
alcoolique, voire alcoolotabagique, extrahé-
patique, tels les cancers et états précancéreux
ORL, bronchiques, œsophagiens, une patho-
logie cardiovasculaire et respiratoire”.
Outre sa toxicité hépatique, l’alcool est reconnu
comme un facteur de risque pour diverses
pathologies, telles que les maladies cardiovas-
culaires et les cancers.
La consommation d’alcool peut être respon-
sable de 3maladies cardiovasculaires : l’HTA,
les troubles du rythme cardiaque et les myo-
cardiopathies avec survenue d’une insuffisance
cardiaque pouvant, en fonction de la fraction
d’éjection résiduelle, contre-indiquer la greffe
hépatique.
Par ailleurs, le tabagisme est plus fréquent chez
les patients atteints d’une cirrhose alcoolique (6).
Au vu de l’effet synergique du tabac et de l’alcool
en termes de carcinogenèse, il est impératif de
réaliser chez ces patients un dépistage appro-
fondi, avant la greffe, des tumeurs pulmonaires
et des voies aérodigestives supérieures (VADS),
qui sont une contre-indication absolue à la TH.
L’effet délétère de l’alcool sur le rein a été maintes
fois décrit. Le retentissement tubulaire rénal
de l’alcool est réversible en cas d’abstinence. À
l’inverse, une néphropathie à immunoglobu-
linesA(IgA) est responsable de lésions glomé-
rulaires irréversibles. Une double greffe foie-rein
est alors nécessaire.
La consommation d’alcool entraîne, outre la
dénutrition liée à la cirrhose, une malnutrition
avec carence protéique et vitaminique. Un état
de dénutrition est corrélé à des complications
infectieuses plus fréquentes et à un séjour en
réanimation prolongé.
Le risque d’accident vasculaire cérébral(AVC)
hémorragique apparait au-delà de 60g/jour
d’éthanol et augmente de manière dose-dépen-
dante. L’encéphalopathie hépatique est souvent
responsable d’un état confusionnel. Cela peut
parfois masquer certaines atteintes neurolo-
giques telles que le syndrome de Korsakoff ou
l’encéphalopathie de Gayet-Wernicke, en général
irréversibles.
Les dommages psychiques de l’alcool, tels que
l’anxiété ou la dépression, peuvent également
se décompenser après la greffe. Des symptômes
dépressifs sont présents chez plus de la moitié
des malades avec cirrhose alcoolique et l’anxiété
généralisée en concerne plus d’un tiers. Après la
greffe, les patients présentant un état dépressif
persistant ont un risque de mortalité multiplié
par2 (7).
Enfin, l’évaluation addictologique est un élément
clé avant transplantation pour maladie alcoo-
lique du foie. Il semble indispensable que la prise
en charge addictologique avant et après la greffe
soit réalisée de façon indépendante du médecin
transplanteur.
Au total, la maladie alcoolique du foie est
véritablement une “maladie systémique”, dans
laquelle une prise en charge multidisciplinaire
est nécessaire quant à la faisabilité d’une greffe
hépatique.
Résultats probants
de la transplantation
hépatique
Si l’on considère les critères usuels de succès
pour la TH que sont la survie, l’absence de rejet
et le taux d’infection, la cirrhose alcoolique est
une bonne indication de TH.
Dès 1988, T.E. Starzl et al. ont montré que les
survies à1 et 3ans des patients greffés pour cir-
rhose alcoolique du foie étaient comparables à
celles des greffés pour cirrhose non alcoo-
lique(8). Cela a été confirmé à maintes reprises
et étendu à la survie à 5ans. La survie chez les
patients transplantés pour cirrhose alcoolique est
respectivement de 84 % à 1an, de 73 % à 5ans,
et de 58 % à 10ans, soit significativement meil-
leure que dans la cirrhose virale ou cryptogé-
nique(figure 2)[9]. La conférence de consensus
de Lyon, en 2005, a d’ailleurs validé “la cirrhose
alcoolique comme une indication de laTH au
même titre que les autres cirrhoses”. Malgré ces
données, il existe encore des réticences à pro-
poser uneTH pour cirrhose alcoolique.
Réticences à adresser
les patients ayant une
cirrhose alcoolique
Aux centres de greffe
Peu d’entre tous les patients porteurs d’une cir-
rhose alcoolique décompensée accèdent effec-
tivement à laTH.
Plusieurs études menées auprès de l’opinion
publique, des patients et des professionnels de
santé montrent que les patients porteurs d’une
cirrhose alcoolique sont considérés comme les
moins prioritaires pour bénéficier d’uneTH,
et ce quelle que soit la pertinence de l’indica-
tion de transplantation(10). La TH n’est pas
envisagée pour de nombreux malades. Tout

Le Courrier des addictions (15) – n ° 2 – Avril-mai-juin-2013
23
d’abord, certains présentent une complication
inaugurale de la cirrhose, entraînant si rapide-
ment le décès que le patient ne peut être évalué.
D’autres présentent une complication de la cir-
rhose mais sont ensuite perdus de vue. Enfin,
parfois, la TH n’est pas proposée aux patients
dont l’alcoolodépendance majeure laisse prévoir
une faible compliance.
Du fait de leur mauvaise image dans la société, les
patients ayant une cirrhose alcoolique sont moins
souvent adressés aux centres de transplantation.
Dans le cadre d’une étude portant sur 199candi-
dats potentiels à une TH pour cirrhose alcoolique
décompensée, seuls41(21 %) ont été adressés à
un centre référent et seuls 15(8 %) ont eu une
évaluation complète avec un bilan avant la greffe
finalisé(11). De plus, suivant l’association de cri-
tères médicaux, chirurgicaux et psychiatriques,
certains programmes récusent plus de 50 % des
cirrhotiques alcooliques adressés pour TH(12).
Au final, seule une petite proportion, estimée à
6 %, des malades susceptibles de décéder d’une
cirrhose alcoolique sont transplantés(13).
Une étude française(14) qui a analysé le devenir
des patients 3ans après une première hospi-
talisation pour cirrhose alcoolique rapporte
que 7 % étaient décédés et que seuls3 % avaient
été transplantés. Il y a beaucoup de candidats
potentiels à une TH pour maladie alcoolique du
foie mais il y a finalement peu d’élus : 9 000décès
par an, et seulement 300TH !
L’enjeu de la rechute
Selon l’HAS, le seul objectif dans l’alcoolo-
dépendance est l’abstinence.
La singularité de la transplantation pour maladie
alcoolique du foie repose sur le risque de reprise
d’une consommation d’alcool après la greffe,
considérée, à tort ou à raison, comme inaccep-
table.
Les données de la littérature retrouvent des taux
de reprise de la consommation d’alcool très dif-
férents après TH, allant de 7 % à 95 % à 3ans chez
les greffés pour maladie alcoolique du foie. Il est
cependant très difficile de comparer ces études
entre elles. En effet, la définition de la rechute varie
selon les études : la plupart utilisent une définition
absolutiste qui considère toute consommation
après la greffe comme une rechute, quelle que
soit la fréquence ou la quantité (15).
D’autres utilisent une définition différenciée qui
consiste à séparer ce qui relève de l’alcoolodé-
pendance telle qu’elle est définie dans le DSM-IV
de la reprise d’une consommation d’alcool carac-
térisée par sa fréquence et sa quantité. Cette
définition distingue ainsi 3 situations cliniques
concernant la consommation d’alcool après la
greffe : l’abstinence, la rechute modérée, et la
rechute sévère(16).
La rechute sévère concerne les patients pré-
sentant des critères d’alcoolodépendance, et/
ou une consommation d’alcool supérieure
à210g par semaine pour les hommes et 140g
par semaine pour les femmes (critères OMS),
et/ou une consommation d’alcool supérieure
à 50g les jours de consommation. Certaines
études ne considèrent que la rechute excessive,
c’est-à-dire supérieure à 30g par jour, ou 40g
par jour, selon les études (17-19).
Enfin, le “slip”, qui est une prise d’alcool isolée ou
lors d’un événement avec poursuite de l’absti-
nence, est un concept récent qui n’est pas consi-
déré comme une rechute dans la définition dif-
férenciée. Il n’y a d’ailleurs aucune différence de
survie significative dans la littérature entre les
patients présentant un épisode de “slip” après
la greffe et les abstinents(17).
Le diagnostic précoce de la rechute est difficile,
car toutes les méthodes de détection, analysées
de façon individuelle, sont imparfaites(20). Cer-
taines études utilisent l’interrogatoire du patient
et de son entourage, d’autres, le questionnaire
anonyme, d’autres encore, l’interrogatoire
téléphonique, avec parfois mise en corrélation
avec les résultats des tests biochimiques(21). Le
diagnostic de rechute est aussi difficile avant la
greffe, les patients pouvant cacher leur consom-
mation alcoolique afin de ne pas être exclus de
la liste d’attente(22).
Enfin, toutes les études citées n’ont pas le même
suivi moyen et plusieurs d’entre elles montrent que
le taux de rechute augmente avec la durée du suivi.
Au final, en tenant compte de toutes ces études,
la rechute alcoolique à 5ans après la TH est
estimée entre 11 et 54 %, avec 7 à 26 % de réci-
dive de consommation excessive(23).
En dehors du champ de la transplantation, il
existe peu de facteurs prédictifs de rechute
chez les patients alcooliques. La greffe peut être
ressentie comme une expérience traumatique
par certains patients et prévenir la rechute. La
culpabilité ressentie par certains patients vis-à-
vis du donneur peut exercer le même effet. Le
facteur prédictif de rechute après TH le plus
souvent rapporté est la durée d’abstinence avant
l’inscription sur liste. Les autres variables iden-
tifiées comme facteurs prédictifs de rechute
sont le jeune âge, les antécédents familiaux
d’alcoolisme, les antécédents personnels de
toxicomanie, un contexte dépressif avec idées
suicidaires et des conditions sociales précaires.
D’autres éléments tels que l’environnement
familial et social et l’absence de pathologie ou
de troubles psychiatriques sont des facteurs
prédictifs d’abstinence, selon une méta-analyse
récente(24).
Au-delà du questionnement moral posé par la
rechute d’un patient transplanté pour maladie
alcoolique du foie, se pose la question des consé-
quences en termes de survie du greffon et du
greffé.
La reprise d’une consommation d’alcool ne
semble pas affecter la survie du greffon ni celle
du patient à 5 ans, lorsqu’on la compare à celle
des patients abstinents(20, 21). En revanche, la
reprise d’une consommation alcoolique exces-
sive a des conséquences sur la survie du patient
à long terme. Initialement, une première étude
a suggéré une diminution significative de la
survie à 10ans chez les patients qui rechutent,
comparativement aux patients abstinents(19).
La surmortalité des patients ayant repris une
consommation excessive d’alcool était imputable
à l’apparition de cancers de novo et aux compli-
cations cardiovasculaires. Cette différence de
survie à long terme, entre patients ayant repris
une consommation excessive et abstinents ou
consommateurs occasionnels était retrouvée
plus tard(17). En 2007, l’impact sur la survie des
tumeurs des VADS de novo était mis en évidence,
avec une supériorité de la survie à 10ans chez les
non-rechuteurs(18). Dernièrement, une étude
française, portant sur 206transplantés pour
maladie alcoolique du foie, a montré une dimi-
nution nette de la survie à 10ans chez les patients
ayant repris une consommation excessive d’alcool.
Les taux de survie à5 et 10ans étaient respective-
ment de 82 % et 49 % chez les patients ayant repris
une consommation excessive contre 86 % et 75 %,
chez les autres patients (p < 0,05) [25].
Intérêt et limites
de la “règle des six mois”
En 1993, la conférence de consensus de Paris
prônait une durée d’abstinence de 3 à 6mois,
voire supérieure à 6mois, avant l’inscription sur
une liste de greffe.
Le rationnel de la “règle des 6mois” est de per-
mettre une récupération de la fonction hépato-
cellulaire avec le sevrage, afin d’éviter une trans-
plantation inutile, de mettre en place une prise
en charge addictologique avec renforcement du
sevrage et d’instaurer une uniformité entre les
différents centres de greffe(10). En 2005, aux
États-Unis, 85 %des centres de TH continuaient
de suivre cette règle(26).
Cependant, aucune étude n’a prouvé l’intérêt
d’une abstinence de 6mois sur les complications
précoces avant, pendant ou après la TH (27).
En 2005, la conférence de consensus de Lyon
stipulait que “la durée de 6mois d’abstinence
avant la TH ne devait plus être une règle intan-
gible et ne devait pas être considérée comme une
condition à elle seule d’accès à la TH”.
En effet, la règle des 6mois est imparfaite,
puisqu’elle inclut des patients qui reprendront
une consommation d’alcool après la greffe et, à
l’inverse, elle exclut des patients qui ne repren-
dront pas de consommation après la greffe. Dans
une étude prospective(14), parmi les patients
ayant une abstinence avant la greffe de 36mois,
seuls 60 % demeuraient abstinents après la greffe.
Une durée d’abstinence de 36mois avant la greffe
prédisait l’abstinence après greffe avec une sensi-
bilité de 80 % mais une spécificité de 40 %. Certes,
chaque mois supplémentaire d’abstinence avant
la greffe diminuait le risque de rechute après la
greffe de33 %, mais il n’était cependant pas pos-

Le Courrier des addictions (15) – n ° 2 – Avril-mai-juin 2013 24
sible d’identifier une durée d’abstinence avant
la greffe assurant une abstinence définitive. En
outre, il n’y a pas ou que peu d’amélioration de
la fonction hépatocellulaire après 3mois d’abs-
tinence (13). Enfin, il est difficile d’estimer véri-
tablement la durée d’abstinence prégreffe. Elle
repose en effet sur l’interrogatoire du patient
et de son entourage, qui souhaite en général
l’intégration du patient dans le projet de greffe
et aura tendance à le protéger.
Situation “extrême” :
l’hépatite alcoolique
aiguë
Les formes graves d’hépatite alcoolique aiguë
sont définies par un score de Maddrey supé-
rieur à32. En l’absence de traitement, plus
de 50 % des patients atteints d’hépatite alcoo-
lique aiguë grave décèdent dans les 6mois qui
suivent le diagnostic. Seules les formes graves
nécessitent un traitement par corticostéroïdes
et/ou pentoxiphylline. L’équipe de Lille a mis
en évidence les facteurs de non-réponse à ce
traitement et a modélisé, à partir de 5variables
indépendantes, le pronostic de ces patients(28).
Ce modèle permet de prédire près de80 % des
décès à 6mois. Les patients non répondeurs à la
corticothérapie ont un risque de décès de 85 %
à 6mois. Il est éthiquement difficile de ne pas
proposer une greffe à ces patients, atteints d’une
hépatite alcoolique aiguë grave et non répon-
deurs au traitement médical, dont la mortalité
est prévisible dès le septième jour. La présence
d’une hépatite alcoolique de découverte fortuite,
lors de l’analyse histologique du foie explanté,
n’a pas, qui plus est, de conséquence en termes
de survie du greffon et du patient ni de rechute
alcoolique après la TH(16). Cependant, l’asso-
ciation fréquente de comorbidités et de défail-
lance multiviscérale chez ces malades, ainsi que
la crainte de la récidive alcoolique par l’équipe
de transplantation et son retentissement sur
l’opinion publique sont autant de freins à la
proposition de TH dans ces cas-là.
Pourtant, une étude française récente multi-
centrique a montré que certains patients haute-
ment sélectionnés présentant une hépatite aiguë
alcoolique corticorésistante, inaugurale, pou-
vaient bénéficier d’une TH avec de bons résultats
en termes de survie à moyen terme et un faible
taux de rechute après la greffe(29). Cependant,
du fait de la gravité du score de MELD de ces
patients, par définition supérieur à30, et de la
pénurie de greffons, il est évident qu’un tel trai-
tement ne peut être réalisé que chez un nombre
restreint de malades.
La pénurie de greffons
Il y toujours actuellement en France 30 % d’op-
position au don d’organes parmi les familles.
De plus, grâce à la prévention routière, on
observe une diminution des états de mort
cérébrale après accidents de la voie publique.
Il y a au final 1 donneur pour 2,3 receveurs
théoriques. Le fait qu’une rechute de la
consommation d’alcool soit possible après TH
pour maladie alcoolique du foie peut avoir un
effet désastreux sur la population générale,
influencée alors par des arguments d’ordre
moral. Cela peut avoir des conséquences
néfastes sur le don d’organes, et aggraver la
situation de pénurie de greffons.
Conclusion
La TH est le traitement validé de la cirrhose
alcoolique décompensée.
Elle est, en 2012, une excellente indication de
transplantation, au même titre que pour les
autres cirrhoses. Cependant, les cancers de novo
et la rechute de la maladie alcoolique affectent
les résultats à long terme. Le bilan avant la greffe,
à la recherche d’une contre-indication, doit être
exhaustif et tenir compte du terrain sous-jacent,
la maladie alcoolique étant une véritable maladie
systémique. Il n’y a plus de durée d’abstinence
minimale requise avant une TH pour maladie
alcoolique du foie. Après la greffe, la prise en
charge addictologique avec le maintien de l’abs-
tinence doit rester une priorité.
v
Références bibliographiques
1. Poynard T, Naveau S, Doffoel M et al. Evaluation of
efficacy of liver transplantation in alcoholic cirrhosis
using matched and simulated controls: 5-year survival.
Multi-centre group. J Hepatol 1999;30(6):1130-7.
2. Vanlemmens C, Di Martino V, Milan C et al. Imme-
diate listing for liver transplantation versus standard
care for Child-Pugh stage B alcoholic cirrhosis: a ran-
domized trial. Ann Intern Med 2009;150(3):153-61.
3.
Wiesner R, Edwards E, Freeman R et al. Model for
end-stage liver disease (MELD) and allocation of donor
livers. Gastroenterology 2003;124(1):91-6.
4.
Merion RM, Schaubel DE, Dykstra DM, Freeman
RB, Port FK, Wolfe RA. e survival benefit of liver
transplantation. Am J Transplant 2005;5(2):307-13.
5.
Lucey MR, Schaubel DE, Guidinger MK, Tome S,
Merion RM. Effect of alcoholic liver disease and hepa-
titis C infection on waiting list and posttransplant
mortality and transplant survival benefit. Hepatology
2009;50:400-6.
6. Jiménez C, Manrique A, Marqués E et al. Incidence
and risk factors for the development of lung tumors
after liver transplantation. Transpl Int 2007;20:57-63.
7. DiMartini A, Dew MA, Chaiffetz D, Fitzgerald MG,
Devera ME, Fontes P. Early trajectories of depressive
symptoms after liver transplantation for alcoholic liver
disease predicts long-term survival. Am J Transplant
2011;11(6):1287-95.
8. Starzl TE, Van iel D, Tzakis AG et al. Orthotopic
liver transplantation for alcoholic cirrhosis. JAMA
1988;260:2542-4.
9. Burra P, Senzolo M, Adam R et al. Liver transplanta-
tion for alcoholic liver disease in Europe: a study from
the ELTR (European Liver Transplant Registry). Am J
Transplant 2010;10(1):138-48.
10.
Neuberger J, Schulz KH, Day C et al. Transplanta-
tion for alcoholic liver disease. J Hepatol 2002;36:130-7.
11. Julapalli VR, Kramer JR, El-Serag HB; American
Association for the Study of Liver Diseases. Evalua-
tion for liver transplantation: adherence to AASLD
referral guidelines in a large Veterans Affairs center.
Liver Transpl 2005;11:1370-8.
12. De Gottardi A, Spahr L, Gelez P et al. A simple score
for predicting alcohol relapse after liver transplantation:
results from 387 patients over 15 years. Arch Intern
Med 2007;167(11):1183-8.
13.
Watt KD, McCashland TM. Transplantation in
the alcoholic patient. Semin Liver Dis 2004;24:249-55.
14. Veldt BJ, Lainé F, Guillygomarc’h A et al. Indica-
tion of liver transplantation in severe alcoholic liver
cirrhosis: quantitative evaluation and optimal timing.
J Hepatol 2002;36(1):93-8.
15. DiMartini A, Day N, Dew MA et al. Alcohol
consumption patterns and predictors of use following
liver transplantation for alcoholic liver disease. Liver
Transpl 2006;12:813-20.
16. Wells JT, Said A, Agni R et al. e impact of acute
alcoholic hepatitis in the explanted recipient liver on
outcome after liver transplantation. Liver Transpl
2007;13:1728-35.
17.
Pfitzmann R, Schwenzer J, Rayes N, Seehofer D,
Neuhaus R, Nüssler NC. Long-term survival and pre-
dictors of relapse after orthotopic liver transplantation
for alcoholic liver disease. Liver Transpl 2007;13(2):197-
205.
18.
Dumortier J, Guillaud O, Adham M et al. Negative
impact of de novo malignancies rather than alcohol
relapse on survival after liver transplantation for alco-
holic cirrhosis: a retrospective analysis of 305 patients in
a single center. Am J Gastroenterol 2007;102(5):1032-41.
19. Cuadrado A, Fábrega E, Casafont F, Pons-Romero
F. Alcohol recidivism impairs long-term patient survival
after orthotopic liver transplantation for alcoholic liver
disease. Liver Transpl 2005;11:420-6.
20. DiMartini A, Weinreib R, Fireman M. Liver
Transplantation in patients with alcohol and other
substance use or disorders. Psychiatr Clin North Am
2002;25:195-209.
21.
Pageaux GP, Bismuth M, Perney P et al. Alcohol
relapse after liver transplantation for alcoholic liver
disease: does it matter? J Hepatol 2003;38:629-34.
22. Tome S, Said A, Lucey MR. Addictive behavior
after solid organ transplantation: what do we know
already and what do we need to know? Liver Transpl
2008;14:127-9.
23.
Kotlyar DS, Burke A, Campbell MS, Weinrieb RM.
A critical review of candidacy for orthotopic liver trans-
plantation in alcoholic liver disease. Am J Gastroenterol
2008;103:734-44.
24.
Dew MA, DiMartini AF, Steel J et al. Meta-analysis
of risk for relapse to substance use after transplanta-
tion of the liver or other solid organs. Liver Transpl
2008;14(2):159-72.
25. Faure S, Herrero A, Jung B et al. Excessive alcohol
consumption after liver transplantation impacts on
long-term survival, whatever the primary indication.
J Hepatol 2012;57(2):306-12.
26. Murray KF, Carithers RL Jr; AASLD. AASLD
practice guidelines: Evaluation of the patient for liver
transplantation. Hepatology 2005;41:1407-32.
27. Weinrieb RM, Van Horn DH, McLellan AT, Lucey
MR. Interpreting the significance of drinking by alcohol-
dependent liver transplant patients: fostering candor is
the key to recovery. Liver Transpl 2000;6:769-76.
28. Louvet A, Naveau S, Abdelnour M et al. e Lille
Model: a new tool for therapeutic strategy in patients
with severe alcoholic hepatitis treated with steroid.
Hepatology 2007;45:1348-54.
29.
Mathurin P, Moreno C, Samuel D et al. Early liver
transplantation for severe alcoholic hepatitis. N Engl J
Med 2011;365:1790-800.
1
/
4
100%