cancer sein investigations radiologiques pre post traitement

Cancer du sein:
Cancer du sein:
les investigations radiologiques
les investigations radiologiques
pré
pré-
-et post
et post-
-traitement
traitement
Prof Jean
Prof Jean-
-Yves Meuwly
Yves Meuwly
Service de Radiodiagnostic et Radiologie
Service de Radiodiagnostic et Radiologie
Interventionnelle, CHUV
Interventionnelle, CHUV-
-Lausanne
Lausanne

Prise en charge du Ca du sein
Prise en charge du Ca du sein
•
•Jusque dans les années 70, mastectomie
Jusque dans les années 70, mastectomie
comme traitement de choix
comme traitement de choix
•
•Introduction ensuite de traitement moins
Introduction ensuite de traitement moins
mutilants
mutilants
–
–Utilisation de la radiothérapie, d’abord seule,
Utilisation de la radiothérapie, d’abord seule,
puis en association avec la chirurgie
puis en association avec la chirurgie
–
–Utilisation de la chimiothérapie adjuvante puis
Utilisation de la chimiothérapie adjuvante puis
néoadjuvante
néoadjuvante
–
–Utilisation de l’hormonothérapie
Utilisation de l’hormonothérapie
Heys SD. Evolution of breast cancer management: focus on neoadjuvant chemotherapy. Breast
Cancer 2001; 8:339-350.
Rustogi A, Budrukkar A, Dinshaw K, Jalali R. Management of locally advanced breast cancer:
evolution and current practice. J Cancer Res Ther 2005; 1:21-30.
Sakorafas GH. Breast cancer surgery--historical evolution, current status and future perspectives.
Acta Oncol 2001; 40:5-18.
Singletary SE. Breast cancer surgery for the 21st century: the continuing evolution of minimally
invasive treatments. Minerva Chir 2006; 61:333-352.

Objectifs de l’évaluation préopératoire
Objectifs de l’évaluation préopératoire
•
•Cartographie de l’extension locale
Cartographie de l’extension locale
•
•Identification des contre
Identification des contre-
-indications au
indications au
traitement conservateur
traitement conservateur
–
–Extension multifocale étendue (> 2 cm)
Extension multifocale étendue (> 2 cm)
–
–Extension multicentrique
Extension multicentrique
–
–Extension intracanalaire extensive
Extension intracanalaire extensive
–
–(Rapport taille tumeur / sein adéquat)
(Rapport taille tumeur / sein adéquat)
•
•Identification d’un carcinome synchrone
Identification d’un carcinome synchrone
controlatéral
controlatéral
Kuhl CK, Braun M. [Magnetic resonance imaging in preoperative staging for breast cancer: pros
and contras]. Radiologe 2008; 48:358-366.
Traitement conservateur chez 80% des femmes

Extension tumorale
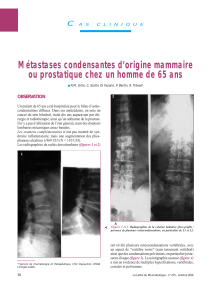
Extension tumorale
Carcinome canalaire invasif étendu à droite
Carcinome canalaire invasif étendu à droite

Reconstruction panoramique
Reconstruction panoramique
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
1
/
49
100%