P - Hepatoweb.com

TUMEURS ENDOCRINES PANCREATIQUES
METASTATIQUES BIEN DIFFERENCIEES
Bertrand DOUSSET
Service de Chirurgie Digestive, Hépato-biliaire et Endocrinienne
Hôpital Cochin
7ème réunion de pathologie digestive 2011

INTRODUCTION
Tumeurs endocrines pancréatiques métastatiques
•TEP fonctionnelles
-Insulinome, Gastrinome
-Vipome, Glucagonome
7ème réunion de pathologie digestive 2011
•TEP non fonctionnelles
•TE digestives (ex tumeurs carcinoïdes)

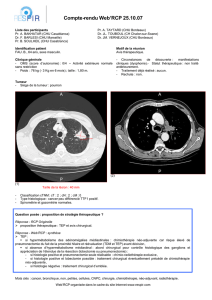
EPIDEMIOLOGIE DES TNE
Incidence Pour 100,000
4.0
6.0
8.0 Homme
Femme
Période
Incidence Pour 100,000
0.0
2.0
4.0
USA1
(SEER) Pays-Bas2
Suède2Suisse2
(Vaud)
Norvège3
Pays
1. Yao J, Hassan M, Phan A, et al. J Clin Oncol. 2008;26:3063-3072. 2. Taal BG, Visser O. Neuroendocrinology. 2004;80(suppl 1):3-7. 3. Hauso O,
Gustafsson BI, Kidd M, et al. Cancer. 2008;113:2655-2664.
2000-2004 1983-1998 1989-1996 1993-2004 1974-1997 1985-1991

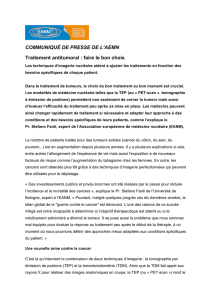
EPIDEMIOLOGIE DES TNE
Incidence pour 100,000
1.40 NET Site
1.20
1.00
0.80
0.60
Poumon
Colon
Intestin grèle
Rectum
Pancreas
Incidence pour 100,000
0.60
0.40
0.20
0
Incidence multipliée par 5 entre 1975 et 2004
Incidence multipliée par 7 dans le registre norvégien
SEER = Surveillance, Epidemiology, and End Results (for malignant NET)
Yao J, Hassan M, Phan A, et al. J Clin Oncol. 2008;26:3063-3072.

EPIDEMIOLOGIE DES TNE
Prevalence
1200000
1100000
65836
103312
cas
1168000
cas
1. Yao J, Hassan M, Phan A, et al. J Clin Oncol. 2008;26:3063-3072. 2. Taal BG, Visser O. Neuroendocrinology. 2004;80(suppl 1):3-7. 3. Hauso O,
Gustafsson BI, Kidd M, et al. Cancer. 2008;113:2655-2664.
Prevalence
100000
0
21427
cas
28664
cas
32353
cas
65836
cas
cas
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
1
/
20
100%