Troubles cognitifs et infection par le virus de l`immunodéficience

90 | La Lettre du Neurologue ̐˫˭ϴ͊˭͉͇͈͉
MISE AU POINT
Troubles cognitifs
et infection par le virus
de l’immunodéficience humaine
Cognitive impairment and HIV
C. Geny*
* CMMR de Montpellier, CHU Gui-
de-Chauliac.
L
´
˺˺´ˈ
̔̕´˫
³̔̕
³´˺
˺´ˈ
̔̕
˺´˨
˺´´
´´˫˺
˺´ˈ´
˺³´´
(Highly Active Antire-
troviral Therapies) [1-5]˫
´´˨˨˺
´
ˈ´˫
˺͍͇͇͌˺
´´˨͈͋ϥ
˨´˺(6, 7)˫
´
´˺´
³̱˨
´´´´
˫˨´
´´
´˨
˨ˈ´
¢ˈ´˭
˫´˨
´˺(7-9)
´ˈ´
´´´
´˫˨´
ˈ´
´͈͌
͇͌ϥ(9)˫´˨˭
ˈ˨
´´
´˫´˺˨
˨´
˨´
˫˨˨
˺˨˺˭
˺´
´˺¢˫˨
´¢´˨
˨´´˨
˺´´˫
Aspects historiques
³´˺´´˨
´
˫
´˨
´˺˺
ˈ´˫˨˫˫˫͈͐͏͍
´
˺“AIDS dementia complex” (The AIDS
dementia complex: I. Clinical features. Ann Neurol
1986;19:517-24)˫͈͈͐͐˨˺
“HIV-associated
dementia” (10)˫
˨˨´˨
´˫
´´´
minor cognitive motor dysfunction˫³
´´͉͇͇͎˺˺˭
Neurology (11)˫

La Lettre du Neurologue ̐˫˭ϴ͊˭͉͇͈͉| 91
Points forts
»Le VIH pénètre dans le SNC dès les premiers stades de l’infection.
»Le tableau sévère de démence associée au VIH est devenu rare en raison de l’efficacité des thérapeu-
tiques combinées.
»La plainte cognitive est fréquente chez le patient VIH, même avec une charge virale nulle.
»
Les troubles cognitifs peuvent être le reflet d’une infection incontrôlée, d’une inflammation chronique,
d’une pathologie vasculaire cérébrale associée, d’un syndrome dépressif ou d’une affection dégénérative
débutante.
»
Les antirétroviraux ont une pénétration intracérébrale variable, actuellement quantifiée par le score CPE.
»
Un bilan cognitif anormal justifie la réalisation d’une IRM, voire d’une ponction lombaire, et peut inciter
à changer de traitement antirétroviral.
Mots-clés
VIH
Trouble neurocognitif
Démence
Dépistage
Vieillissement
Highlights
»
With the introduction of
highly active anti-retroviral
therapy, HIV-associated
dementia disappeared in
clinical practice but the preva-
lence of minor HIV-1 associ-
ated neurocognitive disorder
is increasing even in treated
patients, with well-controlled
infection.
»
These patients complain
about milder memory prob-
lems and slowness, difficulties
in concentration, planning, and
multitasking.
»
In 15-50% of patients,
neuropsychological examina-
tion confirmed subtle cognitive
impairment.
»
The effects of aging or
comorbid conditions as cere-
brovascular disease could
play a role but persistant and
mild immune activation or
toxicity of antiretroviral drugs
is discussed.
»
Patients with memory
complaints must have a cogni-
tive examination. In case of
abnormal results, lumbar punc-
ture, MRI or change of therapy
could be discussed.
Keywords
HAART
Cognitive impairment
HIV-1
Aging
˽³˾̔´̕
˽˺˾˨
˫˺ˈ´
˺´
³´´
³´´´´
˫
´
“HIV-associated neurocognitive disorders”̔̕˨
µ°˽˭
´˾˫´´´´ˈ
˺
´
(tableau I)˫
déficit neurocognitif asymptomatique´ˈ
͉̔´
´
´˺¢
´̕˨´˫
trouble neurocognitif léger
´˫
̱ˈ´ˈ´
˨˭
˫démence associée au VIH
˺´³˺
͉̔ϯ
͉´̕´ˈ´
´˫
̱˨͎
µ´´´´˪˨
̱´˨̱
´˨´̔˭
̕˨´˨
˺
˫˨
˺´˭
´˨´´˨
˫
Physiopathologie
´´³´
³´(8, 9)˫˭
˺´´
´´˺
´˺´
´´˨
˨Ä˺
´´´˨
˺˫
˫´´
´
͈͉͇̔̕´´˺ˉ˫
´͋˪˭
˫˺´
´´͋͌
´Ù´˭
˫´´´
´³˫˺˭
´´˺´˨
´´
˫
˺˺ˉ˭
˺´
˫´´´
ˈ´˨´
´
Tableau I. Classification des troubles neurocognitifs (Antinori et al., 2007).
Performance cognitive Conséquences fonctionnelles
Déficit neurocognitif asymptomatique Perturbation d’au moins 2 domaines
cognitifs (< norme moyenne moins 1 DS)
Pas d’impact sur les activités
de la vie quotidienne
Trouble neurocognitif léger Perturbation d’au moins 2 domaines
cognitifs (< norme moyenne moins 1 DS)
Impact léger
Démence associée au VIH Perturbation d’au moins 2 domaines
cognitifs (< norme moyenne moins 1 DS)
Impact important

92 | La Lettre du Neurologue ̐˫˭ϴ͊˭͉͇͈͉
Troubles cognitifs etinfection par le virus del’immunodéficience humaine
MISE AU POINT
˨´
´´³
´´´˫
˨˺˨
˺˺˭
˫´̔˺³
´̕´
´ÙÆ
´˫
´ˈ´´
nj´
´˨µ
(12-14)˫
nj͉͋
´̔̕[15]˫˺´͋
Ϩ˺Ϩ
(9)˫³´´
´˪
´nj
˺Ƴ´˺ˉ˭
˫
˺˺
˫´˨´
˨´
´´(16, 17)˫
´´
´
´´˫´
˺´´˭
´´
˺˫
Épidémiologie
˺
͍͇͇͌´
´´˺´͉͇͇͏(6)˫˺¢
͊͏˫
͈͋ϥ´˺´´˨
´˺´³˫
´´
´´˨͎͊ϥ
͉ϥ˫˨
´˺
´´̔´͉͇͇͇͇͌̕
͇͇͇͇͌˭
˫´´
´˨´´
˨̱˭
´̔͋ϯ͉͇͇̭
͊
̕˫
˨
ˈ͏͊ϥ
´͇̭͍͌
³˺´˫
´´´
´˫´
´˺´˨´˨
˺¢´´
´˫˨˭
´ˉ͉͇ϥ˫˺´
´´´
´˺
´˫˨´͊ϥ͈͉͐͐˨
͇˨͊͋ϥ͉͇͇͇͇˨͉͋ϥ͉͇͇͊(2)˫
³˺
´͎͌ϥ˺´
(9)˫´
´´
´˨´˨´˫
˺´(CNS HIV Anti-Retroviral Therapy
Effects Research)˨´´´ˈ´˭
˺´
˨´͉͌ϥ
͉ϥ
´³(4)˫˨
´´
(18-21)˫´
˺¢͉̔͋ϥ
͊̚¢˪̛͍͋
͉͈ϥ̕
͍͇˫
³˨͋͐ϥ
Ù˭˨
´´´´͈͈ϥ˫
˺˺¢´˺Æ
˺¢´͇͌
´͊˨͉͍(5)˫˺
´´
´͌(7)˫
´¢´
´
˫˭˺³´
´´˪´͇̔͌ϥ̕˨
³͍̔ϥ̕˨´̔͐ϥ̕˨
̔͋͌ϥ̛̕̚˫
ˈ
˺(17)˫
˨´´
˺
˺ˉ
˨ˈ
´˫

La Lettre du Neurologue ̐˫˭ϴ͊˭͉͇͈͉| 93
MISE AU POINT
Aspects cliniques
´´´´
͈͐͏͇˫´´
³
³˨
˭˫˨
´˨´˭
˺
´´´˨´˫˨
´´´
˫´´
˨´˭
´´˫
Forme classique de démence
associée au VIH
´´´´´³
´͈͐͏͇´
˭
(1, 3, 10)˫˺˺
´
´˭˫
˺´
˺˺´˭
˨
´˨ˈ´˺
˨
´(22)˫ˈ˺´
´˭˨´
´
˺°˫´´˨
˭
´´˫˨ˈ˺
µ˨´˨
µ(23)˫
˨˨
ˈ
tapping˫˨
˨î
´´˫
Déficit neurocognitif léger
´ˈ´
´˭
(11)˫
ˈ´˺˨˺˨
ˈ´
´˫µ´˨
´˨
ˈ´´
(23, 24)˫
ˈˈ´´
´˫
´´˨
˺´˺˫˺
˫
´
´´´˫
˫˨´
ˉ´̔˺̕˨
´̔˺
̛̚̕˨
˺̔̕˫
˺
˨
ˈ´tapping˫
´´´
͉
´˫´
´˺˭
(22, 23)˫˺´
´´
´˫˨´´³˫
³´˨
˫
Diagnostic
´´ˈ´(tableau II)
´ˈ˫˺¢˨
˭˺´
˺͋
´˫˨
µ´
´̔´˨
˨³̕˨ˈ´
Tableau II. Facteurs associés à la survenue d’un trouble neurocognitif lié au VIH.
Liés à l’hôte Liés à l’infection virale
– Faible réserve cognitive
– Insulinorésistance, diabète
– Abus de substances psychotropes
(alcool, cocaïne, héroïne, métamphétamine, etc.)
– Mauvaise observance
– Génome (ApoE, etc.)
– Infection VIH non contrôlée
– Nadir CD4 bas
– Stade C
– Durée de l’infection chronique
– Co-infection VHC
– Variants VIH (?)

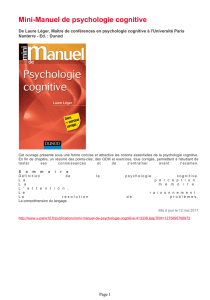
Recherche FDR
Signes neurologiques d’accompagnement
Impact sur les activités
de la vie quotidienne
Bilan de dépistage
Codes, 5 mots, horloge, fluence
Plainte isolée
Tests normaux
Pas de conséquences fonctionnelles
Quelques anomalies
aux tests
FDR+ FDR–
Contexte
psychologique
Bilan
neuropsychologique
MMS pathologique
activités
Prise en charge
FDR Suivi clinique PL/IRM
FDR : facteurs de risque cognitifs ; MMS : Mini-Mental State.
Changement
thérapeutique
–
+
Figure. Algorithme décisionnel chez un patient VIH+ présentant des troubles cognitifs
débutants.
94 | La Lettre du Neurologue ̐˫˭ϴ͊˭͉͇͈͉
Troubles cognitifs etinfection par le virus del’immunodéficience humaine
MISE AU POINT
˫
´˨
´´´ˈ˫
´˺˨
´˫
´´´´
´´˨˺´˭
˨
˫
´´´´´´˺´
´˭
˭˪Multicenter AIDS Cohort
Study ̔̕battery˨ˬ
˺´³
͉
͈͉˫´´´´´µ
´´
˫
L’HIV dementia scale´˭
´˺ˈ
´´˺´
˫´´͋¢
´´̔͋͌̕˨
˺˨´˭
˫L’international HIV dementia scale
͊¢̔´˨´
˨ˈ̕˫´
´
´°
˫
´˫˨
´
³´´
´(6)˪
͌˨˨˺˫
˨˺
´˨
´´ˈ˺´
´
´˫
´figure˫
´
µ´˺³´´
̔˭
˨´´˨̕
´˫µ˨
´˨
´
´˺´´˪
´´¢˨
´˨³˨˨
˨˺´˫
´˺´˺
˺´˫
Apport des examens
paracliniques
˺´´´´
´
˫˺´˭
̔´˭
̕˨˫
˨
´˫´´˨
̔
´´´͉
͈̕[1, 25]˫Ù
´˨´˭˨
˨
´˫´
˺
̱´´´
´˫
´´
´˫´´˨
˭˭˺˫
 6
7
6
7
1
/
7
100%