immunogenicite de la mort cellulaire induite par

1
UNIVERSITE PARIS XI
FACULTE DE MEDECINE PARIS-SUD
THESE
pour obtenir le grade de
DOCTEUR DE L’UNIVERSITE PARIS XI
Champ disciplinaire : Immunologie
Ecole doctorale de rattachement : Cancérologie, Biologie, Médecine, Santé
Présentée et soutenue publiquement par
Laetitia AYMERIC
Le 08 juillet 2011
IMMUNOGENICITE DE LA MORT CELLULAIRE INDUITE
PAR LES CHIMIOTHERAPIES ANTI-CANCEREUSES
Directeur de thèse : Pr. Laurence ZITVOGEL
Composition du jury :
Président
Rapporteur
Rapporteur
Examinateur
Examinateur
Directeur de thèse
Pr. Eric SOLARY
Pr. Muriel MOSER
Pr. Nicolas GLAICHENHAUS
Dr Jenny VALLADEAU
Dr Kamel BENLAGHA
Pr. Laurence ZITVOGEL

2
REMERCIEMENTS
Je tiens à remercier ma directrice de thèse, le professeur Laurence ZITVOGEL, pour m’avoir
accueillie dans son laboratoire, pour sa présence et son dynamisme moteur au quotidien.
Merci également aux docteurs Evelyn ULLRICH, Magali TERME, Grégoire MIGNOT et
Mathieu BONMORT, pour m’avoir aidée à faire mes premiers pas dans le laboratoire, en
ayant pris le temps de m’enseigner le fonctionnement de celui-ci et quelques bases
expérimentales.
Un merci particulier à Sophie VIAUD, aussi serviable que compétente, qui a su m’apporter
de précieux conseils techniques tout au long de ma thèse.
Merci également aux docteurs Nathalie CHAPUT, Sylvie RUSAKIEWICZ et Dalil
HANNANI pour les discussions scientifiques passionnantes que nous avons eues ensembles.
Merci à tous mes collègues qui savent travailler dur dans la bonne humeur et avec un bon état
d’esprit, sans lesquels ma thèse n’aurait pas été la même.
Je tiens à remercier très sincèrement les responsables de l’animalerie de l’IGR (SCEA), M.
Patrick GONIN et Mme Karine SER LE ROUX, pour leur compétence et leur ouverture
d’esprit. Ils ont toujours su concilier au mieux les exigences de leur structure avec nos
travaux scientifiques.
Merci à tous nos collaborateurs pour leur générosité. Un merci particulier au docteur Kamel
BENLAGHA, pour m’avoir fait profiter de son expertise sur les NKT à un moment de ma
thèse.
Enfin, je remercie chacun des membres de mon jury pour avoir accepter d’apporter leur
jugement éclairé à mon travail. Je remercie sincèrement les professeurs Muriel MOSER et
Nicolas GLAICHENHAUS pour avoir accepté la tâche d’évaluer mon rapport de thèse.

3
RESUME
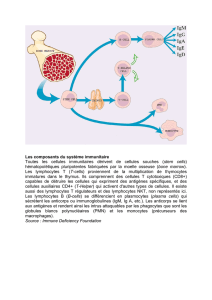
Le développement d’un cancer chez un individu immunocompétent témoigne de
l’inefficacité de ses défenses immunitaires naturelles à entraver la progression tumorale. La
restauration ou l’induction de réponses immunitaires anti-tumorales efficaces sont des enjeux
majeurs des stratégies thérapeutiques actuelles. En plus des immunothérapies classiques,
visant à activer le système immunitaire des patients contre leurs tumeurs, les thérapies
conventionnelles, telles que les chimiothérapies et la radiothérapie, peuvent avoir des effets
immunostimulants, en parallèle de leur effet directement cytotoxique sur les cellules
tumorales. Parmi celles-ci, les anthracyclines, l’oxaliplatine et la radiothérapie sont
notamment capables d’induire une mort cellulaire immunogène. L’efficacité thérapeutique de
ces traitements dépend de l’activation de lymphocytes T (LT) CD8 anti-tumoraux,
producteurs d’interféron-gamma (IFN-γ). En utilisant des modèles murins de tumeurs
transplantées, nous montrons que le traitement des cellules tumorales par des drogues
immunogènes induit la libération d’adénosine triphosphate (ATP) dans le milieu extra-
cellulaire. Ce signal de danger endogène se lie à son récepteur P2RX7 sur les cellules
dendritiques et permet la formation de l’inflammasome NLRP3/ASC/pro-caspase 1,
conduisant à l’activation protéolytique de la caspase 1, qui active la pro-interleukine-1β (pro-
IL-1β) en interleukine-1β (IL-1β). L’IL-1β peut directement agir sur les LT CD8 pour
faciliter leur polarisation vers un phénotype de lymphocytes T cytotoxiques de type 1 (Tc1).
De plus, le traitement de tumeurs établies par des drogues immunogènes induit une
production d’IL-17A (IL-17) dans le lit tumoral, au cours de la première semaine suivant le
traitement. Les LT gamma delta (LTγδ) sont les principaux producteurs de cette cytokine
dans nos modèles. Ces cellules s’accumulent transitoirement dans la tumeur dès le troisième
jour suivant le traitement et leur taux est parfaitement corrélé à celui des LT CD8 producteurs
d’IFN-γ tumoraux. Comme l’IFN-γ, l’IL-17 et les LTγδ sont nécessaires à l’efficacité
thérapeutique des drogues immunogènes. L’IL-1β produite par les cellules dendritiques
exposées à des corps apoptotiques immunogènes stimule directement la production d’IL-17
par les LTγδ. Ces travaux ont contribué à identifier l’ATP extra-cellulaire comme un
déterminant moléculaire de l’immunogénicité des cellules tumorales exposées à certaines
thérapies anti-cancéreuses conventionnelles. De plus, nous montrons que les traitements
cytotoxiques classiques peuvent moduler l’environnement immunitaire dans le lit tumoral, et
contribuer à remplacer une inflammation chronique et immunosuppressive en une
inflammation aigüe et immunogène. L’étude des interactions entre le système immunitaire et
les thérapies anti-cancéreuses conventionnelles est nécessaire pour utiliser ces traitements de
manière plus rationnelle, en les combinant par exemple à des immunothérapies plus
classiques.

4
ABREVIATIONS
ADN : acide désoxyribonucléique
ARN : acide ribonucléique
ASC : “apoptosis-associated speck-like protein”
ATP : adénosine triphosphate
BM-DC : cellules dendritiques dérivées de la moëlle osseuse
CD : “cluster of differentiation”
CMH : complexe majeur d’histocompatibilité
COX-2 : cyclo-oxygénase 2
HMGB1 : ”high mobility group box 1”
IFN : interféron
IL: interleukine
IL-1R : récepteur à l’interleukine 1
IL-1RA : antagoniste naturel du récepteur à l’interleukine 1
IL-17 : interleukine 17A
LB : lymphocyte(s) B
LT : lymphocyte(s) T
LTγδ : lymphocytes T gamma delta
MDSC : cellules myéloïdes immatures immunosupressives
NFκB : “nuclear factor-κB”
NLRP3 : “NLR family, pyrin domain-containing 3”
NO : oxyde nitrique
pDC : cellules dendritiques plasmocytoïdes
TAM : macrophages associés aux tumeurs
Tc : lymphocytes T cytotoxiques
TGF-β : “transforming growth factor-β”
Th : lymphocyte T CD4 auxiliaire
TLR : récepteur de type Toll
Treg : lymphocytes T régulateurs
VEGF : “vascular endothelial growth factor”
WT : non mutées

5
SOMMAIRE
REMERCIEMENTS ............................................................................................................... 2
RESUME .................................................................................................................................. 3
ABREVIATIONS ..................................................................................................................... 4
SOMMAIRE ............................................................................................................................. 5
INTRODUCTION.................................................................................................................... 6
1 La présence d’un danger : une condition nécessaire à l’activation du système immunitaire ?
............................................................................................................................................................ 6
1.1 La théorie du danger et les signaux de danger ................................................................................... 6
1.2 Les réponses immunitaires au danger ................................................................................................. 9
2 Les réponses immunitaires naturelles dans le cancer ............................................................... 19
2.1 Les tumeurs : tolérance ou immunité ? ............................................................................................. 19
2.2 Environnement tumoral et immunosuppression .............................................................................. 31
3 Les solutions thérapeutiques pour activer des réponses immunitaires anti-tumorales
efficaces ............................................................................................................................................ 39
3.1 L’utilisation de ligands de TLR en immunothérapie anti-cancéreuse ........................................... 39
3.2 Effets immunostimulants des thérapies anti-cancéreuses conventionnelles ................................... 43
4 Contexte d’étude et objectifs de la thèse .................................................................................... 51
4.1 Les mécanismes moléculaires de l’immunogénicité de la mort cellulaire induite par certaines
thérapies anti-cancéreuses conventionnelles ........................................................................................... 51
4.2 Problématiques de la thèse ................................................................................................................. 53
MATERIEL ET METHODES ............................................................................................. 54
RESULTATS .......................................................................................................................... 57
1 Rôle de l’activation de l’inflammasome NLRP3 et de la production d’IL-1β par les cellules
dendritiques dans l’efficacité des chimiothérapies immunogènes .............................................. 57
2 Rôle des LTγδ producteurs d’IL-17 dans l’efficacité thérapeutique de thérapies anti-
cancéreuses conventionelles ........................................................................................................... 60
DISCUSSION ......................................................................................................................... 62
1 Importance des modèles de tumeurs établies ............................................................................ 62
2 Rôle de l’ATP extra-cellulaire dans le développement de réponses immunitaires spécifiques
.......................................................................................................................................................... 63
3 Rôle de l’IL-1β dans le développement de réponses Th1 et Tc1 spécifiques .......................... 65
4 Rôle de l’IL-17 dans le développement de réponses Th1 et Tc1 spécifiques .......................... 66
5 Rôle de l’IL-17 et de l’IL-1β dans la progression tumorale ..................................................... 69
CONCLUSION ET PERSPECTIVES ................................................................................. 70
REFERENCES ....................................................................................................................... 73
ANNEXES .............................................................................................................................. 88
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
1
/
126
100%
![Poster CIMNA journée CHOISIR [PPT - 8 Mo ]](http://s1.studylibfr.com/store/data/003496163_1-211ccc570e9e2c72f5d6b6c5d46b9530-300x300.png)