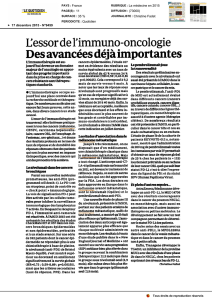
E. PUJADE-LAURAINE - L`immunothérapie dans le

L’immunologie
fait peur

Baby B
King Thymus VIII
CD 8
Princess Thymus IV
CD 4
La Famille Lymphocyte

La reconnaissance de l’antigène par le
macrophage ou la cellule dendritique
Et alors!
Je sais! C’est
du non-moi!
Je l’apporte à
la famille T
Oups! Qu’est-ce
que c’est que ça?
macrophage Antigene
Cellule
dendritique

La présentation de l’antigène
CD 8
Antigène
Cellule
dendritique
King Thymus VIII
Récepteur
cellule T
B27
CD28

CD 8
CD 8
King Thymus VIII
CD 8
La réaction
immune
Récepteur
cellule T
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
1
/
45
100%