61st YEAR - 6 1 e ANNÉE - World Health Organization

W kfy Eputem. Rec • R ti& e epukm hebd. 1986,61,101-108 No. 14
WORLD HEALTH ORGANIZATION
GENEVA
ORGANISATION MONDIALE DE LA SANTÉ
GENÈVE
WEEKLY EPIDEMIOLOGICAL RECORD
RELEVÉ ÉPIDÉMIOLOGIQUE HEBDOMADAIRE
Telegraphic Adtbas: EPIDNATIONS GENEVA Telex 27S21 Adreae UUgraphupie EPIDNAT10NS GENÈVE Télex 27821
Automatic Tdcx Reply Soviet Service summnimiic de lépooie p«r id g
Telex 28150 Geneva with ZCZC and ENGL torn reply in English Télex 28150 Genève suivi de ZCÏC el BRAN pour une réponse en fonçais
4 APRIL 1986 61st YEAR -61e ANNÉE 4 AVRIL 1986
EXPANDED PROGRAMME ON IMMUNIZATION
Neonatal tetanus mortality surveys
In d o n e s ia , - Few countries in the less developed world have a
clear picture of their incidence of neonatal tetanus. During the past
year 3 surveys completed in different provinces of Indonesia have
provided data to supplement earlier studies.1 The studies earned
out in rural areas of Sumatera Barat, Aceh and Nusatenggara
Barat, using the WHO cluster survey methods, found incidences of
9,21 and 17 per 1000 live births respectively. This may be com
pared with the average level of 11 per 1 000 estimated from a
survey of 19 provinces in 1982 which used the same methodology.1
In these 3 areas the infant mortality rate was estimated at 103-129
per 1 000 live births, of which neonatal mortality represented over
50% and neonatal tetanus 20-25%.
Among the most significant findings were:
(i) Tetanus toxoid immunization of the mothers during their
pregnancy' varied from a low 3% in Nusatenggara Barat to
18% in rural Sumatera Barat, even though up to 90% of
mothers had attended prenatal care and other health services
during pregnancy on 2 or more occasions.
(lij Births attended by trained traditional birth attendants
(dukun) suit had a death rate up to 5 per 1 000 live births.
(tu) Deliveries supervised by trained traditional birth attendants
often had incidences little different from those supervised by
untrained ones.
(iv) Male children had incidence rates up to 3 times the female
rate, indicating that there may be a difference in the practices
associated with cord care, as the rate was almost equal
amongst non-neonatal tetanus deaths.
Other findings included:
(i) The incidence of neonatal tetanus varied significantly with
the level of education of the mother, but in some areas this
effect w'as seen only for women with higher secondary
level.
(ii) The highest incidence rates were associated with the use of
knife or bamboo for cutting the umbilical cord; conversely,
lower rates were associated with the use of scissors from the
UNICEF kits.
(ui) Treatment of the cord stump with either antiseptic or tradi
tional application did not result m marked differences in the
neonatal tetanus rate.
1 Sec No 8, 1983. pp, 56-57.
PROGRAMME ÉLARGI DE VACCINATION
Enquêtes sur la mortalité par tétanos néonatal
In d o n é sie . - Rares sont les pays du monde en développement qui ont
une idée exacte de l’incidence du tétanos néonatal sur leur territoire. Trois
enquêtes achevées l’an dernier dans 3 provinces d’Indonésie ont fourni
des informations qui complètent des éludes antérieures.1 Ces enquêtes,
menées dans les zones rurales de Sumatera Barat, d’Aceh et de Nusa
tenggara Barat au moyen de la méthode OMS de sondage par grappes, ont
révélé respectivement des taux d’incidence de 9, 21 et 17 pour 1000
naissances vivantes, chiffres que l’on peut rapprocher du taux moyen de
11 pour 1 000 obtenu lors d’une enquête effectuée en 1982 dans 19 pro
vinces selon la même méthode.1 Dans ces 3 régions, le taux de mortalité
infantile a été estimé à 103-129 pour 1000 naissances vivantes dont plus
de 50% sont imputables à la mortalité néonatale et 20 à 25% au tétanos
néonatal.
Voici quelques-unes des principales constatations faites au cours de ces
enquêtes:
0 Les taux de vaccination des femmes enceintes par l’anatoxine téta
nique oscillent entre 3% (Nusatenggara Barat) et 18% (zones rurales
de Sumatera Barat), alors que jusqu’à 90% des mères avaient consulté
les services de soins prénatals et d’autres services de santé 2 fois ou
davantage durant leur grossesse.
u) Les accouchements assurés par des accoucheuses traditionnelles for
mées (dukun) correspondaient encore à un taux de mortalité de 5 pour
1 000 naissances vivantes.
ni) L’incidence du tétanos néonatal correspondant aux accouchements
assurés par des accoucheuses traditionnelles formées ne se différencie
guère de celle qui correspond aux accouchements assurés par des
accoucheuses traditionnelles non formées.
iv) Chez les enfants de sexe masculin, les taux d’incidence sont 3 fois plus
élevés que chez les enfants de sexe féminin, ce qui donne à penser que
les méthodes utilisées pour la section du cordon ombilical pourraient
différer selon le sexe, car dans le cas des décès non liés au tétanos
néonatal, les taux de mortalité sont presque idenuques.
On a également fait les observations suivantes:
i) L’incidence du tétanos néonatal varie de façon significative selon le
degré d’instruction de la mère. En certains endroits cependant, il n’en
va ainsi que pour les femmes ayant suivi un enseignement du niveau
secondaire supérieur.
il) Les taux d'incidence les plus élevés corespondent aux cas où l’on s’est
servi'd’un couteau ou d’un bambou pour sectionner le cordon ombi
lical et les tauxies plus faibles à ceux où l’on avait utilisé des ciseaux
provenant des trousses, du F1SE.
ni) Le fait d’employer un antiseptique plutôt qu’un produit traditionnel
pour traiter la section du cordon ombilicaî n’a pas entraîné de grandes
différences entre les taux de tétanos néonatal.
1 Voir N° 8, 1983 pp. 56-57
Epidemiological notes contained m this issue:
Dengue, epidemiological surveillance, Expanded Pro-
gramme on Immunization, influenza, nosocomial infections,
tetanus.
List of newly infected areas, p. 108.
Informations épidémiologiques contenues dans ce numéro*
Dengue, grippe, infections nosocomiales, programme élargi de vac
cination, surveillance épidémiologique, tétanos.
Liste des zones nouvellement infectées, p. 108.

Relevé êpidèm hebd. N® 14 -4 avril 1986
4j{ld^£picitni Rec No 14-4 April 1986 - 102
itvj Neonaxal tetanus rates were higher for those infants where
There was a dearly disturbing persistent high level of neonatal
tetanus in these areas and many opportunities to protect mothers
against this disease during pregnancy are being missed. Major
recommendations from these studies were that mass campaigns be
conducted amongst women of childbearing age, starting in those
districts withyhç btàhjrit^nri^epfe^fln foci tljjfo has. started ihthe
Province of Nu^tfenggara-BaFat where'bveF'90%’coverage was-
obtained for the second round of tetanus toxoid. A feature of this
rprararomewgs^n ^tepsw^çgl|fo^cj£ça#pn£f|prt and^he useof
JB P ftW ^ h k a t JtdÀ^tnlaS% i»u|à d%lfiF.organizâtibjB'
conduct of the campaign.1) A call was also made to review the
training and supervision of traditional birth attendants.
As pointed out in the reports, the elimination of neonatal
tetanus-from these- provinces would reduce theînfant'morfaTîty
; rate substantially. PeThaps the most disiurbihg leatures of these
studies W Ihe' ldw’coverage-rby tetanus 'toxoid; despite the
riûmérbüscontacts most mbthèfsnad with health services during
pregnancy. and the. JM ingjn some areas, thaï the use.of trained,
traditional birth attendants had no effect in reducing the incidence
of neonâtal tetanus. These findings and the subsequent initial
~suctessftJt'massprogrammedireciedai women-0fchildbearing age-
make a compelling case for such approaches to be the first step in
accelerating .the fïgtu against neonatal tetanu^
iv) Les taux de tétanos néonatal étaient plus élevés lorsqu’il y avait eu
précédemment un décès dans la même fratrie.
Dans les régions étudiées, on a observé un taux élevé et constant de
tétanos néonatal vraiment préoccupant, de nombreuses possibilités de
protéger les mères contre la maladie durant leur grossesse étant négligées.
L’une des recommandations majeures que l’on a pu lâire sur la base de ces
études concerne l’organisation de campagnes de masse chez les femmes
jeq âge-de. procréer, en commençant par les districts où l’incidence est la
"‘plus élevée. (De fait, on a entamé ces campagnes dans la province de
Nusatenggara Barat où une couverture de plus de 90% a été obtenue pour
. la-seconde dose d’anatoxine tétanique; Le programme comporte un vaste
L
elfiart d’éducation pour la santé et a recours aux autorités locales ainsi
qu’à des groupes de femmes pour l’organisation et l’exécution de la cam
pagne. ‘) Il a également été recommandé de réexaminer la formation et la
supervision des accoucheuses traditionnelles.
Comme il est indiqué dans les rapports, l’élimination du tétanos néo-
Tiafol dans ces provinces réduirait fortement la mortalité infaniile.Les
constatations les plus préoccupantes de ces études sont peut-être celles
qui ont trait à la faible couverture vaccinale antitétanique, malgré les
nombreux contacts que la plupart des mères ont eus au cours de leur
grossesse avec les services de sanié, et au foit qu’en certains endroits,
l’intervention d’accoucheuses traditionnelles formées n’a entraîné
aucune réduction de l’incidence du tétanos néonatal. Ces constatations et
' la réussite initiale du programme de masse organisé ultérieurement à
l’intention des femmes en âge de procréer plaident puissamment en
faveur de ces approches qui doivent constituer une première étape dans
l’intensification de la lutte contre le tétanos néonatal.
' See No '46'*1 SBSfpp 353-hS4. 1 Voir N» 46,1985, pp. 353-354.
(Based pn/D’après:. A report, from, the Ministry of Health/Un rapport du Ministère de la Santé, 1985.)
Un it e d S i a t es o f A m e r ic a .-T he NationafNosocomial Infec- '
tions Study (NNIS) has collected and analysed ;da ta-on the fre- “
quencÿ of nosocomial infections in United States hospitals since
I970:'This reportprovides descriptive data on nosocomial infec
tions in' a sample of hospitals in }983i‘ ' ■' 11 : ' * ‘ -
Materials and methods
• Hospitals participating in NNIS conducted active hospital-wide1
surveillance using uniform definitions of nosocomial infectionsi
During 1983,54hospitals regularly reported data ta the Centers for
Disease Control (CDCX For each nosocomial .infection detected,
the fotlowing information was' reported: site of infection, date of
onset, whether the mfecuon was associated vrith a surgical proce
dure, the pathogen(s) isolated, occurrence:of secondary bade-.
raem%anri/nicrqbial susceptibility çfbaçterial pathogens, service
of the pattern,; and, for those patients who, died with a nosocomial,
mfecuon, the relationship of the infection todéUth. Jo addition, the
hospitals reported the njjmber of pauenfs discharged each month
From the 6 primary services: medicine, surgery, obstetrics, gynap-
çbjogy, paediatrics, andmçwbofn.
Data are, recorded on. standardised foriqps, which are sent to
pDC'éacb mçnth. When the fyttjare received gt CDC, they are
coded, entered into a computer, and edited before being ana
lysed. ~
Results
The NNIS sample. The hospitals participating in NNJS are not a
probability sampleof hospitals inthe-Uriited States; however, the
54 hospitals that reported data regularly in'1-983 range in sizé fronr
80 m over 1 200 beds, are located throughout the country, and
include hospitals owned by state and local governments, as well as
by profit and n cun-profit organizations; -The geographicafdistnbu-
hon of the 54 hospitals among'the 4 regions of-thecountry-
(Northeast, North Central, South, Wesifis raughlythesame as for
all 6 053 hospitals included in the American Hospital Association
Annual Survey of hospitals. Hospitals affiliated with medical,
schools, referred, to .as teaching hpspitgls, ape .still greatly over-,
represented' among the NNIS hospitals ; 56% (30 out of 54) of th,e
NNIS hospitals are teaching hospitals, whereas only 14% ofthe
hospitals across the country are affiliated with medical schools.
Similarly, the 54 NNIS hospitals tend to be large, with a median
size of407 beds, compared with a median size of only 1J O beds for
the 6’053"hospitals. \
The.infcct.ionratesifauiiiberiifhQspitalracquireduifeaionsper,
1000 patients discharged) wereinghest ra the large teaching hos
pitals and lowest in the non-teaching hospitals (Table 1), as were
the infection rates on eaqh pfjjte 6 sçryicçs (Tapie 2J. In jdJ 3
Irospitalcategoncs. ihèM eâioâ rate-.was highest, oiuhè siirgery.
Et a t s-U n is D’A m é r iq u e . - Dans le cadre d’une étude nationale sur les
infections nosocomiales (NNIS), on a recueilli et analysé les données
1 relatives à la fréquence de ces infections aux Etats-Unis depuis 1970. Le
présent rapport contient des données descriptives sur les infections noso
comiales survenues dans un échantillon d’hôpitaux en 1983.
Données et méthodes
Les établissements hospitaliers participant à l’étude ont exercé une
surveillance active à l’échelon de l’hôpital en utilisant des définitions
uniformes des infections nosocomiales. En 1983, 54 hôpitaux ont régu
lièrement communiqué des données aux Centers for Disease Control
(CDC). Pour chaque infection nosocomiale décelée, les informations sui
vantes ont été communiquées: localisation de l'infection, date d’appan-
tion de l’infection, infection associée ou non à une intervention chirur
gicale, agent(s) paihogène(s) isolé(s), apparition d’une bactériémie secon
daire, sensibilité aux antimicrobiens des bactéries pathogènes, service
dans lequel était hospitalisé le patient, et pour les patients décédés d’une
infection nosocomiale, relation entre l’infection et le décès. En outre, les
hôpitaux ont notifié le nombre de patients quittant chaque mois 6 ser
vices essentiels; médecine, chirurgie, obstétrique, gynécologie, pédiatrie
et néonatalogie.
Les données sont enregistrées sur des formulaires normalisés, qui sont
envoyés chaque mois aux CDC. Lorsque les CDC reçoivent les données,
elles sont codées, mises sur ordinateur, puis vérifiées avant d’être analy
sées.
Résultats
L’échantillon NNIS. Les hôpitaux participant à l’étude ne représenteni
pas un échantillon aléatoire des hôpitaux des Etats-Unis. Néanmoins, les
54 hôpitaux qui ont régulièrement communiqué des données en 1983
comptaient de 80 à plus de 1 200 lits, étaient situés dans tout le pays et
comprenaient des hôpitaux gérés par l’Etat et le gouvernement local, ou
par des organisations privées, à but lucratif ou non. La répartition géo
graphique des 54 hôpitaux entre les 4grandes régions du pays (Nord-Est,
Centre-Nord, Sud, Ouest)était plus ou moins la même que celle des 6 053
hôpitaux recensés par 1'American Hospital Association Annual Survey of
Hospitals. Les hôpitaux affiliés à des écoles de médecine, ci-après
dénommés hôpitaux universitaires, sont cependant considérablement
surreprésentés parmi les hôpitaux couverts par la NNIS ; en effet, 56% (30
sur 54) des hôpitaux couverts par l’étude sont des hôpitaux universitaires,
alors que 14% seulement des hôpitaux du pays sont affiliés à des écoles de
médecine. De même, les 54 hôpitaux couverts par l’étude sont générale
ment grands (ils comptent en moyenne 407 lits), alors que la capacité
moyenne des 6 053 hôpitaux américains est de 110 lits seulement.
Les taux d’infection (nombre d’infections nosocomiales pour 1 000
patients quittant l’hôpital) ont été les plus élevés dans les grands hôpitaux
universitaires et les plus bas dans les hôpitaux qui n’étaient pas des
établissements d’enseignement (Tableau l), ce qui était vrai également
. .pourchacun des ô.services (Tableau 2). Dansles 3 catégories d’hôpitaux.

Wkty Epidem Rec No. 14-4 Apnl 1986 Relevé èputem kebà N° Î4 - 4 avril 1986- 103 -
service, followed generally by medicine, gynaecology, and obstet
rics. The one exception was in the small teaching hospitals, w here
the infection rates on the medicine and gynaecology services were
similar. Lowest infection rates were reported on the newborn and
paediatrics services.
le taux étau le plus élevé dans te service de chirurgie, également suivi par
la mêdccme, la gynécologie et l'obstétrique. 'La seule exception se situait
parmi les petits hôpitaux universitaires, où les taux d'infection pour les
services de médecine et de gynécologie étaient très voisins. Les taux les
plus bas ont été signalés dans les services de néonatalogie et de pédia
trie
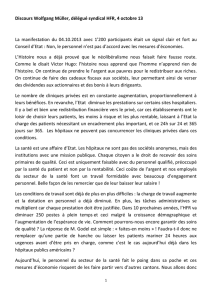
Table 1 Nosocomial infections: infection rates'* by hospital category, United States of America, 1983
Tableau 1. Infections nosocomiales: taux d’infection* par catégorie d’hôpitaux, Etats-Unis d'Amérique, 1983
Hospital category
Catégorie d'bôpaaux Infections Discharges
Patients
quittant
rhôpitai
Rate
Taux
Non-teaching — Non universitaires . 6 845 281122 24.4
Small teachmg — Peuis hôpitaux universi
taires
............................
...
............................
7 875 255 601 ' 30.8 •
Large teachmg — Grands hôpitaux universi
taires ................................
..
...................
13 528 328 559 . 41.2-
T o ta l
..................................................................
28 248 865 282 32.7
* Case, per 1 000.discharges. — Nombre de cas pour 1 000 paucob amtUun I'hpaiUit . . ‘
Table 2. Nosocomial infections: infection rates* by hospital category and service^ United States of America, 1983
Tableau 2 Infections nosocomiales: taux d'infection* par catégorie d’hôpitaux, et par service, Etats-Unis d’Amérique, 1983
Service
Catégorie d’hôpilau* Surgery
Chirargie Medicine
Médecine Gynaecology
Gynécologie Obstetrics
Obstétrique Newborn
Néonatalogie Paediatrics
Pediatne
Non-teaching - Non universi
taires ................................... 32 1 27.8 135 10.3 8.9 ? ?
Small teachmg - Petits hôpitaux
universitaires
.........................
42.6 35.0 35.6 15.6 11.0 11,0
Large teachmg — Grands hôpi
taux universitaires .... 57 5 47.5 31,4 16.9 18.4 ' 16.8
T o t a l......................................... 443 37.1 27.4 14.7 13.4 1 U
1 Cases per l 000 discharges. — Nombre de cas pour 1 000 patients quittant l’hôpitaL
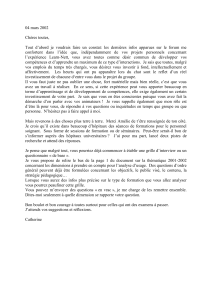
The urinary tract was the most frequent site of infection, fol
lowed by surgical wounds and lower respiratory tract in all 3 hos
pital categories (Table 3). On each service and for each sue of
infection, the infection rates were highest in the large teaching
hospitals and lowest in the non-teaching hospitals.
In all 3 hospital categories, infections of the urinary tract, sur
gical wounds, and lower respiratory tract accounted for over 70%
of the infections (Table 4). Primary bacieraemia accounted for a
higher percentage of infections in the large teaching hospitals than
in the other hospitals.
Combined rates by service and site. In general, the site-specific
infection rate within each service was highest in the large hospitals
and lowest in the non-teaching hospitals (Table 5). The site-
specific infection rates by service show that for each hospital cate
gory, urinary tract infections occurred predominantly on the sur
gery, medicine, and gynaecology services. Surgical wound infec
tions occurred predominantly on the surgery, obstetrics, and
gynaecology services. Lower respiratory infections occurred pre
dominantly on the medicine and surgery services. Primary bacte-
raemia occurred primarily on the surgery, medicine, and newborn
services. Cutaneous infections occurred primarily on the newborn
service
La localisation de l’infection ta plus fréquente était les voies urinaires,
suivie par les plaies chirurgicales et les voies respiratoires inférieures, et
cela pour les 3 catégories d’hôpitaux (Tableau 3k Pour chaque service et
pour chaque localisauon, les taux d'infection étaient les plus eleves dans
les grands hôpitaux universitaires et les plus bas dans les hôpitaux qui
n’etaient pas des établissements d’enseignement.
Dans les'3 catégories d’hôpitaux, les infections des voies urinaires, des
plaies chirurgicales et des voies respiratoires inférieures représentaient
plus de 70% des infecuons (Tableau 4). La bactériémie primaire était
responsable d’un pourcentage plus élevé d’infections dans les grands
hôpitaux universitaires que dans les autres hôpitaux.
Taux combinés par service et par localisation. En général, le taux
d’infection par localisation à l'intérieur d’un même service 'était plus
élevé dans les grands hôpitaux et plus faible dans les ,hôpitaux non uni
versitaires (Tableau 5j. tes taux d’infection par localisation et par service
montrent que pour-chaque-catégorie d’hôpital, les infecuons des voies
unnaires surviennent principalement dans les services de chirurgie, de
médecine et de gynécologie. Les infections des plaies chirurgicales sur
viennent principalement dans les services de chirurgie, d’obstétnque et
de gynécologie. Les infections des voies respiratoires inférieures survien
nent principalement dans -les services de médecine et de chirurgie. La
bactériémie primaire survient principalement dans les services de chi
rurgie, de médecine et de néonatalogie.Les infections cutanées survien
nent principalement dans les services de néonatalogie.
' Table 3. Nosocomial infections: infection rates* by hospital category and site of infection, United States of America, 1983
Tableau 3. Infections nosocomiales: taux d’infection* par catégorie d’hôpital et par localisation de l’infection, Etats-Unis d’Amériqne, 1983
-lafecuon
Hospital category
Catégorie d'hôpitaux Urinary
tract
Voies
unnaires
Surgical
wound
Plaies
chirurgicales
Lower
respiratory tract
Voies
respiratoires
inierietues
Cutaneous
infection
Infecuons- -
Primary
bacteremia
Racienémie
primaire
-Other -
Autres
• 1’ ;
Non-teaching — Non universi
taires
...................
, , > . * ti.i 4.0 4.1 1.3 1.3 2.5
Small teachmg — Petits hôpitaux
universitaires.......................... 13.0 6.3 4,6 , .1.5 1.7- >3.9 , .
Large teaching — Grands hppi- -■ '2.7
- 'i,' * -
taux universitaires
................
15.0 7.0 7.5 ' 3.8 5.2 ‘
T o ta l
............................................
13.1 5.8 5 5 • IS ’ ' ' 2.4 3.9
1 Cases per 1 000 discharges. - Nombre de cas pour 1000 panons quittant l'hôpital.

H'kiy Epultm JUc No, 14-4 Apnl 1986 - 104 - Relrw epidém. Hebd N" 14-4 avril 1986
Table 4. Nosocomial infections: percentage of site-specific infections by hospital category, United States of America, 1983
Tableau 4. infwtinnc nosocomiales: pourcentage d’infections par localisation et par catégorie d’hôpitaux, Etats-Unis d'Amérique, 1983
Hospital category - Catégorie d’hôpitaux
Infection Non-
ifgghing
'Non
universitaire
Small
teaching
Petits
hôpitaux
universitaires
Large
tisaehing
Grands
hôpitaux
universitaires
Total
Urinary tract — Voies urinaires 45.8 42.2 36.3 40.2
Surgical wound — Plaies chirur- 16.8 17.7
gicales................ -
................
16.1 20.4
Lower respiratory tract — Voies 18.4 16.9»
respiratoires inférieures . . .
Cutaneous infection — Infec- 16.5 14.8
u o q s cutanées . . . . . . . . 5.8 5.3 9.1 75
Primary bacteraetnia — Bacté- 4.8 6.6 5.9
némie primaire
...................
5.7
Other — Autres
................
...
. 10.1 12.5 12.7 12.0
Table 5, Nosocomial infections: site-specific infection rates* by service, United States of America, 1983
Tableau 5 Infections nosocomiales: taux d’infection» par localisation et par service, Etats-Unis d’Amérique, 1983
/ Non-teaching hospitals — Hôpitaux non universitaires
Service
Infection
Unnary
tract
Voies
urinaires
Surgical
wound
Plaies
chirurgicales
Lower
respiratory
tract
Voies
respiratoires
inferieures
Primary
bacieraenua
Bactcnemie
primaire
Cutaneous
infection
Infections
cutanées
Other
Autres
Ail sites
Toutes
localisations
Surgery — C hirurgie
................
...
. . . 13.3 8.9 5.1 1.3 1.2 2 3 32.1
Medicine — Médecine
.........................
15 3 0.4 5.6 2*2 1.3 3.1 27.8
Gynaecology — Gynécologie
................
8.2 3.8 0,4 6.2 0.2 0.7 13 5
Obstetrics — Obstétrique . . . . . . . 2.8 4.1 02 02 0,3 2.7 10.3
Paediatrics - P é d ia trie
.........................
—0.5 0.5 0.1 0.3 0.8 2 2
Newborn - Néonatalogie . . . . . . . . 0.3 0.1 1.4 1.3 3.8 2 2 i.9
T o ta l
...............................................
... 11J 4.0 4.1 13 1.4 2 S 24.4
2. Small teaching hospitals — Petits hôpitaux universitaires
Service
Infection
Unnary
tract
Voies
urinaires
Surgical
wound
Plaies
chirurgicales
Lower
respiratory tract
Voies
respiratoires
inferieures
Primary
bacteraenua
Bactenemie
primaire
Cutaneous
infection
Infections
cutanées
Other
Autres
AU
sites
Toutes
localisations
Surgery — Chirurgie................................ 16.0 13.5 6.6 1.6 1.0 3.9 42.6
Medicine — Médecine
.........................
19.1 0.7 67 2.6 1.5 4.5 35 0
Gynaecology — Gynécologie . . . . . . 20.6 11.8 08 0.4 0.3 1.6 35 6
Obstetrics — O bstétrique
......................
3.4 8.0 0.7 0.3 0.4 2.7 156
Paediatrics — P é d ia trie
.........................
1.4 0.6 1.3 1.6 1.1 5,0 11.0
Newborn — Néonatalogie
......................
0.4 0.2 0.8 1.3 4.8 3.4 11.0
T o ta l ............................................................ 138 6 3 4A 1.7 15 3S3 05
3, Large teaching hospitals — Grands hôpitaux universitaires
Service
Infection
Unnary
tract
Voies
urinaires
Surgical
wound
Plaies
chirurgicales
Lower
respiratory tract
Voies
respiratoires
inferieures
Primary
baeieraemia
Bactenemie
primaire
Cutaneous
infection
Infections
cutanées
Other
Autres
Ail
sites
Toutes
localisations
Surgery — Chirurgie
.
...............................
19.2 15.5 10.1 4.3 2.9 5.5 57.5
Medicine — Médecine
.........................
21.1 1.3 10.2 5.S 2.9 6.4 47.5
Gynaecology — Gynécologie
.............
16.2 7.7 3.0 1.1 0.7 2 2 314
Obstetrics — O bstétriq ue
......................
4.7 7.5 - 0,4 • 0.7 0.6 3.0 16.9
Paediatrics — Pédiatrie . . . . . . . . . 2.2 2.4 3.2 2.4 2.3 4.4 16.8
Newborn— N éonatalogie
......................
0.7 0.4 4.0 2.6 5.5 5.2 18.4
T o tal............................................................ 158 75 75 38 2.7 55 41.2
* Cases per 1 000 discharges. — Nombre de cas pour 1 000 patients quittant Thopital.
Pathogens. Of the 28 248 infections reported, 66% were caused
by single pathogens, and 1.9% were caused by multiple pathogens.
No pathogen was identifiedin 5% of the infections, and no culture
was obtained in 10%. Of the 8S% of infections in which pathogens
were identified, 86% were caused by aerobic bacteria, 2% by an
aerobic bacteria, and 7% by fungi.
Agents pathogènes. Sur les 28 248 infections signalées, 66% ont été
causées par un seul pathogène et 19% par plusieurs. Dans 5% des cas,
aucun agent pathogène n’a été identifié et dans 10% des cas aucune culture
n’a été obtenue. Sur les 85% d’infections pour lesquelles on a identifié
l’agent pathogène, 86% étaient imputables à des bactéries aérobies, 2% à
des bactéries anaérobies et 7% à des champignons.

Wkty Epuiem, Rec Na 14-4 April 1986 105 - Reine eputem. kebd. N“ 14 - 4 avril 1986
Viruses, protozoa, and parasites accounted together for S% of
the infections of known etiology. Escherichia, colt. Staphylococcus
aureus, enterococci and Pseudomonas aeruginosa were the most
frequently reported pathogens. E. coli was the most frequently
reported pathogen on the medicine, surgery, obstetrics, and gynae
cology services; S. aureus was the most frequently reported
pathogen on the paediatrics and newborn services. P. aeruginosa
was the second most frequently identified pathogen on both the
medicine and surgery services and was less frequent on the other 4
services; enterococci were the second most frequently identified
pathogens on the obstetrics and gynaecology services and third
most frequently identified on the medicine and surgery services;
coagulase-negative staphylococci were the second most frequently
identified pathogens on the paediatrics and newborn services and
fourth most frequently identified on the obstetrics service.
The pathogens most frequently associated with infections,
according to site, were as follows; urinary tract, E coli-, surgical
wound, S. aureus-, lower respiratory tract, S. aeruginosa-, primary
bacteraemia, coagulase-negative staphylococci Other associated
pathogens are also shown in Table 6, by order of frequency.
Les virus, protozoaires et parasites étaient responsables de 5% des
infections d'étiologie connue. Escherichia coli, Staphylococcus aureus, les
entérocoques et Pseudomonas aeruginosa ont été les agents pathogènes
les plus souvent signalés. E. coli a été l’agent pathogène le plus souvent
signalé dans les services de médecine, de chirurgie, d'obstétrique et de
gynécologie et S', aureus dans les services de pédiatrie et de néonatalogie.
P. aeruginosa a été le second agent pathogène le plus souvent identifié
dans les services de médecine et chirurgie et le moins fréquent dans les 4
autres services; les entérocoques ont été le second agent pathogène iden
tifié dans les services d’obstétnque et de gynécologie et le troisième dans
les services de médecine et de chirurgie ; les staphylocoques dépourvus de
coagulase ont été le second agent pathogène le plus souvent identifié dans
les services de pédiatrie et de néonatalogie et le quatrième dans les ser
vices d’obstétnque.
Les agents pathogènes le plus fréquemment associés aux infections,
selon leur localisation, ont été les suivants : voies urinaires, E. coli ; plaies
chirurgicales, S. aureus; voies respiratoires inferieures, P. aeruginosa-,
bactériémie primaire, staphylocoques dépouvus de coagulase. D’autres
agents pathogènes associés aux infections sont également indiqués au
Tableau 6. par ordre de fréquence.
Table 6. Nosocomial infections: pathogens associated with site-specific infections, ranked by frequency of occurrence.
United States of America, 1983
Tableau 6. Infections nosocomiales: agents pathogènes associés aux infections, selon leur localisation, par ordre de fréquence,
Etats-Unis d’Amérique, 1983
Infection £ coti Enterococci
Entérocoques P aeruginosa Klebsiella
SPP- froieus
SPP S aureus
Coag. neg.
staph,
dépourvus
de coag.
Enterobacter
0PP*
Unnary tract — Voies urinaires ........... i 2345_,
Surgical wound — Plaies chirurgicales .......
Lower respiratory tract — Voies respiratoires infë- 325——14—
neures
.........................
......
.
............................
5—13_2
_
4
Primary bacteraemia — Bactériémie primaire . . . 3 5 —4-21-
Table 7 Nosocomial infections: infections reported as having caused or contributed to death of patients, 1983
Tableau 7. Infections nosocomiales: infections notifiées comme ayant provoqué la mort ou y ayant contribué, 1983
Hospital category
Caiegone d'hôpitaux
Number of
infections
Nombre
d'infections
Percentage that
caused
death
Pourcentage
d'mfecuons
ayant
provoqué la
mort
Percentage that
contributed
to death
Pourcentage
d'infections
ayant
contribué à
la mort
Non-teaching — Non universitaires 6 728 0.5 3.7
Small teaching — Petits hôpitaux universi-
taires ............................................................ 7 140 1.3 4.0
Large teaching — Grands hôpitaux universi-
tairas ............................................................ 12 228 0.8 3.4
T o ta l................................................................... 26 096 0 9 3.6
Mortality. Of the 54 NNIS hospitals, 50 (representing > 50% of
hospitalized patients with fatal nosocomial infections) assessed
and reported the relationship of infection to death. These 50 hos
pitals reported mortality data on a total of 26 096 infections.
Approximately 1% of infections were reported to have caused
death, and 3.6% were reported to have contributed to death
(Table 7). Infections were more often reported to , cause or
contribute to death in the teaching hospitals.
Mortalité. Sur les 54 hôpitaux couverts par l’étude, 50 (représentant
plus de 50% des patients hospitalisés décédés d’infections nosocomiales)
ont diagnostiqué et signalé une relation de cause à effet entre l’infection et
le décès. Ces 50 hôpitaux ont communiqué des données de mortalité pour
un total de 26 096 infections. Environ 1% des infections ont été notifiées
comme ayant provoqué la mort et 3,6% comme y ayant contribué
(Tableau 7). Les hôpitaux universitaires ont notifié un plus grand nombre
d’infections ayant provoqué la mon ou y ayant contribué.
(Based on/D’après; P AH O Epidemiological Bulletin, Vol. 6, No. 3, 1985.)
EPIDEMIOLOGICAL SURVEILLANCE
“Sentinel” notification system
Sw i t z e r l a n d . — With the support of the Fœderatto medicorum
helmicorum (FMH) and the Société suisse de médecine générale
(SSMG), the “sentinel” notification system will be introduced
throughout the country next May. It will comprise as representa
tive as possible a network of practitioners who will report con
tinuously to a central office on certain selected morbidity indica
tors. This system should be able to remedy the present lack of
information about primary health care.
"Seminel” notification system is the term used to designate a
network of medical practices, mainly general practitioners, intern
ists and paediatricians, who maintain contact with a central office
and supply regular and standardized reports on morbidity indica
tors for certain diseases. With the help of this network of “look-out
posts” it is to some extent possible to follow the development of
trends in non-hospital practice and to assess the importance of a
variety of medical problems which,affect the population.
SURVEILLANCE ÉPIDÉMIOLOGIQUE
Système de déclaration «sentinelle»
Su is se. — Le système de déclaration «sentinelle», avec l'appui de la
Fœderatio medtcorum helvettcorum (FMH) et de la Société suisse de
médecine générale (SSMG), sera introduit dans l’ensemble du pays en
mai prochain. Il sera constitué d’un réseau aussi représentatif que pos
sible de praticiens qui déclareront de manière continue à une centrale des
indicateurs de morbidité déterminés. Ce système devrait permettre de
combler la lacune d’information qui existe sur le plan des soins de santé
primaires.
On entend par système de déclaration «sentinelle» un réseau de cabi
nets médicaux, principalement des généralistes, des internistes et des
pédiatres, reliés à une centrale assurant un enregistrement continu et
standardisé d’indicateurs de morbidité de maladies déterminées. Grâce à
ce réseau de «postes de garde» il est possible d’analyser jusqu’à un certain
point l’évolution des tendances au niveau de la pratique ambulatoire et
d’évaluer l’importance de divers problèmes médicaux touchant la popu
lation.
1
/
5
100%