Nouveaux anticoagulant et fibrillation atriale

Nouveaux anticoagulants
et fibrillation atriale
non valvulaire
Thierry Pepersack MD PhD
CHU St Pierre, Bruxelles
JEPU Sept 2015

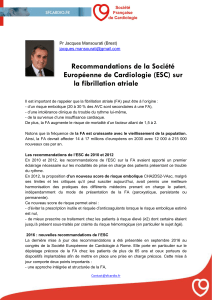
FA: une condition gériatrique?
•La prévalence de la FA double
chaque décennie après 50
ans
•A augmenté
indépendamment du
vieillissement de la
population
•Sa prévalence va encore
augmenter!
•Problème de Santé Publique
•coût des complications
Heeringa J, van der Kuip DA, Hofman A, Kors JA, van Herpen G, Stricker BH, et al. Prevalence, incidence and lifetime risk of atrial
fibrillation: the Rotterdam study. European heart journal. 2006;27(8):949-53.

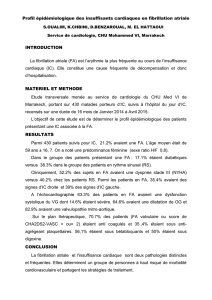
Présentation clinique
•Asymptomatique
•Découverte
–fortuite
•Palpitations moins souvent ressenties % jeunes
–en présence de Défaillance Cardiaque, AVC
•Précipitée par infection, pneumonie, chirurgie,
hyperthyroïdie, EP, …

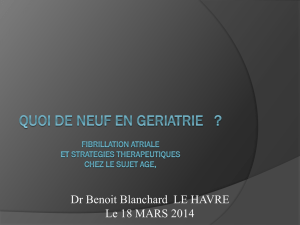
Complications de la FA
•La présence d’une FA augmente le risque de
décès de 50 à 90% par rapport à des sujets du
même âge en rythme sinusal.
•La mortalité est d’autant plus élevée qu’il
existe une cardiopathie ou une insuffisance
cardiaque associée.

La FA: la grande faucheuse!
•Régression logistique après ajustement pour:
–âge, HTA, tabac, diabète, HVG, infarctus,
défaillance congestive, valvulopathie, AVC ou AIT
•Le risque de mortalité est de
–1.5 (95%CI, 1.2-1.8) chez hommes
–1.9 (95% CI, 1.5-2.2) chez femmes
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
1
/
43
100%