Vitiligo: Clinical Aspects, Immunopathogenesis, Therapy
Telechargé par
adilalaissaoui

Vitiligo: Focus on Clinical Aspects,
Immunopathogenesis, and Therapy
Katia Boniface
1
&Julien Seneschal
1,2
&Mauro Picardo
3
&Alain Taïeb
1,2,4
Published online: 6 July 2017
#Springer Science+Business Media, LLC 2017
Abstract Vitiligo is an acquired chronic depigmenting disorder
of the skin, with an estimated prevalence of 0.5% of the general
population, characterized by the development of white macules
resulting from a loss of epidermal melanocytes. The nomencla-
ture has been revised after an extensive international work within
the vitiligo global issues consensus conference, and vitiligo (for-
merly non-segmental vitiligo) is now a consensus umbrella term
for all forms of generalized vitiligo. Two other subsets of vitiligo
are segmental vitiligo and unclassified/undetermined vitiligo,
which corresponds to focal disease and rare variants. A series
of hypopigmented disorders may masquerade as vitiligo, and
some of them need to be ruled out by specific procedures includ-
ing a skin biopsy. Multiple mechanisms are involved in melano-
cyte disappearance, namely genetic predisposition, environmen-
tal triggers, metabolic abnormalities, impaired renewal, and al-
tered inflammatory and immune responses. The auto-immune/
inflammatory theory is the leading hypothesis because (1) vitili-
go is often associated with autoimmune diseases; (2) most viti-
ligo susceptibility loci identified through genome-wide associa-
tion studies encode immunomodulatory proteins; and (3)
prominent immune cell infiltrates are found in the perilesional
margin of actively depigmenting skin. However, other studies
support melanocyte intrinsic abnormalities with poor adaptation
of melanocytes to stressors leading to melanocyte instability in
the basal layer, and release of danger signals important for the
activation of the immune system. Recent progress in the under-
standing of immune pathomechanisms opens interesting per-
spectives for innovative treatment strategies. The proof of con-
cept in humans of targeting of the IFNγ/Th1 pathway is much
awaited. The interplay between oxidative stress and altered im-
mune responses suggests that additional strategies aiming at lim-
iting type I interferon activation pathway as background stabi-
lizing therapies could be an interesting approach in vitiligo. This
review covers classification and clinical aspects, pathophysiolo-
gy with emphasis on immunopathogenesis, and promising ther-
apeutic approaches.
Keywords Vitiligo .Review .Pathophysiology .
Immunopathology .Therapy
Abbreviations
CRT Calreticulin
CTL Cytotoxic T cells
ER Endoplasmic reticulum
HSP Heat shock protein
IFN Interferon
IL Interleukin
NK Natural killer
pDCs Plasmacytoid dendritic cells
PRR Pathogen recognition receptors
ROS Reactiveoxygenspecies
SV Segmental vitiligo
TLR Toll-like receptors
Katia Boniface and Julien Seneschal equally contributed to this work.
*Alain Taïeb
alain.taieb@chu-bordeaux.fr
1
INSERM U1035, ATIP-AVENIR, Université de Bordeaux,
Bordeaux, France
2
Department of Dermatology and Paediatric Dermatology, National
Centre for Rare Skin disorders, Saint-André and Pellegrin Hospital,
Bordeaux, France
3
San Gallicano Institute, Rome, Italy
4
Department of Dermatology and Pediatric Dermatology, St André
Hospital, Bordeaux University Hospitals, 1 Rue Jean Burguet,
33075 Bordeaux, France
Clinic Rev Allerg Immunol (2018) 54:52–67
DOI 10.1007/s12016-017-8622-7

TNF Tumour necrosis factor
Tregs Regulatory T cells
UPR Unfolded protein response
VGICC Vitiligo Global Issues Consensus Conference
VETF Vitiligo European task force
Introduction
Vitiligo is the most common skin depigmenting disorder
resulting from a selective loss of epidermal melanocytes, and
affects around 0.5% of the world population [1,2]. Both sexes
are equally affected, and there are no apparent differences in
rates of occurrence according to phototype or race. Twenty-
five percent of cases are children with disease onset before the
age of 10, the age of onset in paediatric series varies from 4 to
8 years. Very early onset, as young as 3 months, is acknowl-
edged. The existence of true ‘congenital vitiligo’remains con-
troversial. In fair-skinned individuals, vitiligo patches are usu-
ally detected only after the first exposure of the skin to sun-
light, following the first summer of life. The percentage of
segmental vitiligo (SV) is higher in children compared to
adults, whatever the ethnic background, suggesting a mosaic
skin developmental predisposition [1]. The prevalence of SV
in childhood varies from 4.6 to 32.5% in published reports [3].
Vitiligo is a complex disease, associating genetic and envi-
ronmental factors together with metabolic and immune alter-
ations. Abnormalities leading to impaired melanocyte regen-
eration and/or proliferation suggest a primary defect of mela-
nocytes [4]. However, a major role of silent inflammation and
autoimmunity is demonstrable, in particular during the pro-
gressive phase of the disease [5–10]. Since neither immune
nor non-immune mechanisms in isolation can sufficiently ex-
plain all parts of this complex disease, a convergence of com-
bined biochemical, environmental, and immunological factors
in genetically predisposed patients has been proposed as a
unifying background to the pathophysiology of vitiligo [11].
This review summarizes classification, clinical aspects, and
current as well as promising novel therapeutic approaches.
The role of the immune response in vitiligo pathogenesis is
particularly emphasized because of its therapeutic implica-
tions in relation to current drug development.
Classification
The nomenclature has been revised after an extensive interna-
tional work within the Vitiligo Global Issues Consensus
Conference (VGICC) [12]. Vitiligo is now a consensus um-
brella term for all forms of generalized vitiligo (formerly des-
ignated in the international nomenclature as non-segmental
vitiligo) defined as an acquired chronic pigmentation disorder
characterized by white patches, most often symmetrical,
increasing in size progressively or during flares with time,
corresponding histologically to a substantial loss of function-
ing epidermal pigment cells and, usually in a second time, of
hair follicle melanocytes. Two other subsets of vitiligo are SV,
and unclassified/undetermined vitiligo, which corresponds to
focal disease and rare variants. A series of hypopigmented
disorders may masquerade as vitiligo, and some of them need
to be ruled out by specific procedures including a skin biopsy
[1,2].
Clinical Aspects
Vitiligo Subsets
Generalized Common Vitiligo
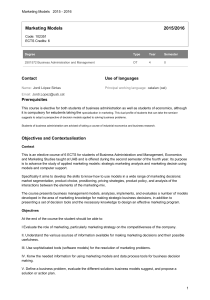
This most common form of vitiligo (Fig. 1a) is characterized
by milky-white macules involving multiple parts of the body,
most often in a symmetrical pattern. Skin hypopigmentation is
usually asymptomatic, but a minority of patients mention pre-
ceding mild pruritus. The disease can start at any site of the
body, but the fingers, hands, and face are frequently the initial
sites. Clinical markers of progression are important to detect
such as pinpoint depigmentation and fuzzy limits of white
macules (Fig. 1b). Obtaining a validated comprehensive list
of validated clinical markers of progression is currently an
international goal, because history-based scores such as
VIDA [13] are considered as grossly inaccurate.
Depigmentation of scars (Fig. 1c) is a common manifestation
of the Koebner’s phenomenon (mechanical induction of the
disease, also by friction or chronic pressure by clothing or
daily activities). Koebner’s phenomenon is usually contempo-
rary of disease flares [14]. Stable lesions are well demarcated
(Fig. 1d).
Mixed vitiligo is a recently described, mostly paediatric
subtype, with segmental involvement preceding typical gen-
eralized vitiligo [15], now included as a subset of vitiligo in
the VGICC classification. The presence of leukotrichia and
halo nevi have been noted as predictors of passage to mixed
vitiligo in patients with SV. Mixed vitiligo may exist in adults
but is probably frequently masked by widespread bilateral
lesions.
Acrofacial Vitiligo
In acrofacial vitiligo, the involved sites are usually limited to
face, head, hands, and feet. A distinctive feature is depigmen-
tation of the distal fingers and facial orifices. It may later
include other body sites, resulting in typical generalized viti-
ligo. Acrofacial vitiligo was shown to be more frequent in
adult onset cases of vitiligo in a large series studies using latent
class analysis [16].
Clinic Rev Allerg Immunol (2018) 54:52–67 53

Vitiligo Universalis
Vitiligo universalis (Fig. 1e) is a rare presentation of vitiligo. It
is the most extensive form of the disease and generally occurs
in adulthood. ‘Universalis’is generally used when depigmen-
tation is virtually universal (80–90% of body surface), but
some pigmentation may be still present, and hairs partially
spared. Whereas this diagnosis is easy in dark-skinned indi-
viduals, it may be more challenging in fair-skinned
individuals.
Segmental Vitiligo
Mono-segmental vitiligo is the most common form of SV,
referring to the presence of one or more white depigmented
macules distributed on one side of the body, usually respecting
the midline (although some lesions may partly cross the mid-
line), early follicular involvement (leukotrichia), and rapid
development over a few weeks or months, and overall
protracted course, but secondary extension remains possible
in a given segment sometimes years after. The shape of SV
Fig. 1 Clinical features of vitiligo. aVitiligo/non-segmental vitiligo. b
Confetti lesions and fuzzy borders in rapidly progressive vitiligo. c
Koebner’s phenomenon on abdominal surgical scars, in a case of progres-
sive vitiligo. dStable vitiligo with well-demarcated macules. eExtensive
vitiligo progressing towards universal vitiligo. fSegmental vitiligo, large
blaschkolinear pattern. gSegmental vitiligo, checkerboard pattern, with
evidence of follicular repigmentation after phototherapy. hVitiligo
‘ponctué’/leucoderma punctate. iHypochromic vitiligo (Courtesy Dr.
Silvia Moretti, Florence). jFollicular vitiligo
54 Clinic Rev Allerg Immunol (2018) 54:52–67

lesions may recapitulate some developmental patterns such as
large band Blaschko lines (Fig. 1f). The long held neural the-
ory based on possible dermatomal distribution is challenged
by many exceptions. The aetiology of the SV pattern remains
overall elusive. Rarely, multiple segmental lesions occur si-
multaneously or not distributed either unilaterally or bilateral-
ly. A clear segmental distribution of the lesions with midline
demarcation, together with the associated features described
in mono-segmental cases (leukotrichia, protracted course),
distinguishes this diagnosis versus vitiligo in bilateral cases.
As in vitiligo, repigmentation may occur, usually under com-
bined therapy (see below), according to a marginal, follicular,
or mixed pattern (Fig. 1g).
Unclassified and Rare Variants
The VGICC classification suggests that focal cutaneous or
mucosal vitiligo (defined as small isolated patch that does
not fit a segmental distribution, and which has not evolved
into vitiligo after a period of at least 2 years) should be until
better consensus on nature and course left within the category
undetermined⁄unclassified vitiligo. Some rare variants are
discussed below.
Vitiligo ponctué/punctata
Lesions present as sharply demarcated depigmented
punctiform 1- to 1.5-mm macules involving any area of the
body (Fig. 1h), and has to be distinguished histopathologically
from guttate hypomelanosis, a common condition with no loss
of melanocytes situated on chronically sun exposed sites such
as the legs and forearms.
Vitiligo Minor/Hypochromic Vitiligo
This disease seems to affect only dark-skinned individuals
(Fig. 1i). ‘Minor’refers to a partial defect in pigmentation.
The relation to true vitiligo comes from pathology and coex-
istence with more typical vitiligo macules. Cutaneous T cell
lymphoma needs to be ruled out by repeated biopsies with
molecular studies of clonality, and this diagnosis cannot be
made without a long-term follow-up [17].
Follicular Vitiligo
This designation refers to a form recently described in a young
black patient of generalized vitiligo that primarily involved
the pigment cell follicular reservoir with limited skin involve-
ment, contrasting with marked generalized hair whitening [18]
(Fig. 1j). As noted later in a small series of patients, contrary to
what occurs in common vitiligo, cutaneous depigmentation
follows hair depigmentation which is situated not only in
vitiliginous areas but also in areas with clinically normal-
appearing skin [19].
Immunopathogenesis of Vitiligo
Intrinsic Abnormalities of Melanocytes and Keratinocytes
Several in vitro and in vivo studies have revealed an altered
redox status, with the presence of oxidative stress in cultured
melanocytes coupled with an increased susceptibility to pro-
oxidant agents [20,21]. Elevated levels of reactive oxygen
species (ROS) have been observed in lesional and non-
lesional skin of vitiligo. The increased ROS production by
melanocytes could result from an external stress, such as ul-
traviolet (UV) radiation exposure or chemical damage
(monobenzone or other phenols). A wide range of metabolic
pathways leads to the uncontrolled generation of ROS, and
several lines of evidence suggest that mitochondria could be
the main source of ROS in vitiligo [22,23]. ROS can also
create a pro-inflammatory environment that will contribute
to the activation of the immune system [24]. Moreover, vitili-
go melanocytes, probably as a consequence of increased in-
tracellular oxidative stress, present abnormalities of signal
transduction pathways compatible with a condition of stress-
induced premature senescence-like phenotype. This is charac-
terized by the production of many proteins among the
senescence-associated secretory phenotypes, including the
production of pro-inflammatory cytokines as interleukin
(IL)-6, matrix metalloproteinase 3 (MMP3), cyclooxygen-
ase-2, insulin-like growth factor-binding protein 3 (IGFB3),
and IGFBP7 [25]. In addition, recent observations showed
that melanocyte exposure to chemical agents (4-TBP—4-ter-
tiary butyl phenol—and MBEH—monobenzyl ether of hy-
droquinone) known to trigger vitiligo induces the disruption
of the folding machinery of the endoplasmic reticulum (ER),
leading to the accumulation of immature proteins and
resulting in the activation of the unfolded protein response
(UPR) [26]. UPR activation results in transient attenuation
of protein synthesis, increased capacity for protein trafficking
through the ER, protein folding transport, and increased pro-
tein degradative pathways, including ER-associated degrada-
tion (ERAD) and autophagy. If these adaptive mechanisms
cannot resolve the protein-folding defect, as in vitiligo, cells
enter apoptosis. The UPR comprises three parallel signalling
branches: PRKR-like ER kinase (PERK)-eukaryotic transla-
tion initiation factor 2α(eiF2α) pathway, activating transcrip-
tion factor 6α(ATF6α), and the inositol-requiring enzyme-1
(IRE1)–X-box-binding protein 1 (XBP1). Genome-wide link-
age analysis followed by a sequencing study in a Chinese
population with vitiligo identified XBP1 as a candidate gene
for vitiligo predisposition, which was then confirmed in a
vitiligo Caucasian cohort [27–29]. More recently, He et al.
Clinic Rev Allerg Immunol (2018) 54:52–67 55

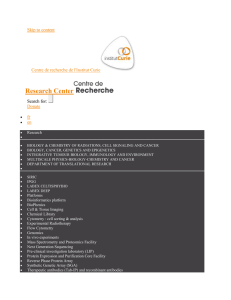
demonstrated that vitiligo melanocytes are more sensitive to
oxidative stress and autophagy, through the impairment of the
nuclear factor E2-related factor 2 (Nrf2) protein, a critical
transcription factor protecting cells from oxidative stress
[30](Fig.2). It is also important to note that Nrf2 is involved
in the UPR activation and acts as a direct PERK substrate.
Fig. 2 Immunopathogenesis of vitiligo. In a predisposed patient,
melanocytes present abnormalities that will lead to the release of
DAMPs and inflammatory cytokines that will contribute to activation of
theinnateimmuneresponseandsubsequently to adaptive T cell
responses, through activation of T
RM
cells that reside in the skin and
recruitment of T
EM
expressing CXCR3 and/or CCR6. These T cell sub-
sets will produce soluble factors (in particular TNFαand IFNγ) involved
in melanocyte loss and development of white patches
56 Clinic Rev Allerg Immunol (2018) 54:52–67
 6
7
8
9
10
11
12
13
14
15
16
17
6
7
8
9
10
11
12
13
14
15
16
17
1
/
17
100%