Lire l'article complet

33
La Lettre du Gynécologue - n° 313 - juin 2006
e cancer du col est un problème de santé mondial.
Chez les femmes, il est le deuxième cancer le plus fré-
quemment rencontré après le cancer du sein (1). Il
représente une cause majeure de décès dans le monde entier et
particulièrement dans les pays en voie de développement où le
dépistage n’est pas aussi pratiqué que dans les pays industriali-
sés. Cependant, malgré le fait que le dépistage cytologique du
cancer du col soit disponible dans les pays développés et que
celui-ci ait largement réduit l’incidence du cancer du col invasif,
le cancer du col localement avancé demeure un problème majeur
pour les cancérologues qui sont toujours à la recherche de nou-
veaux traitements plus efficaces.
Le traitement du cancer du col > 4 cm a été redéfini au cours des
dix dernières années. Deux options thérapeutiques sont propo-
sées : chimio-radiothérapie (CRT) ou chimiothérapie néoadju-
vante (CTN). Une étude randomisée européenne comparant la
CRT et la CTN est actuellement en cours. Néanmoins, la CRT
est considérée comme le traitement de référence du cancer du col
de stade ≥IB2 selon la classification FIGO par de nombreuses
équipes nord-américaines et européennes. La chirurgie radicale
est systématiquement pratiquée après traitement néoadjuvant
chez les patientes soumises à une CTN. Concernant les patientes
traitées par CRT, il n’a toujours pas été clairement défini quelle
est la place de ce que l’on considère comme une chirurgie totale
et quelles sont les procédures et modalités pratiques à mettre en
place après la radiothérapie. Dans la littérature, les résultats de la
chirurgie totale chez des patientes traitées par CRT et présentant
encore de gros reliquats résiduels à l’issue de la radiothérapie
sont rares. Afin d’étudier les résultats de la chirurgie totale, nous
avons décidé d’effectuer une analyse rétrospective permettant
d’évaluer les résultats obtenus chez les patientes après chirurgie
pelvienne consécutive, intervention en principe justifiée chez les
patientes ayant un reliquat tumoral à l’issue de la radiothérapie.
PATIENTES ET MÉTHODES
Les résultats concernant 75 femmes traitées par une CRT sui-
vie d’une chirurgie pelvienne pour un cancer du col localement
avancé entre janvier 1999 et octobre 2002 ont été examinés.
Les patientes retenues pour cette analyse présentaient les
caractéristiques cliniques suivantes :
•
•Tumeur de stade IB2 ou II selon la classification FIGO 1995.
•
•Sous-type histologique : carcinome épidermoïde, adénocarci-
nome ou tumeur adénosquameuse (toutes les lames histologiques
ont été examinées par le même anatomopathologiste).
•
•Toutes les patientes ont eu une radiographie thoracique ini-
tiale et une imagerie par résonance magnétique (IRM) ou une
IRM pelvienne avec tomodensitométrie abdomino-pelvienne
(scanner). La taille de la tumeur a été évaluée sur la base de
l’examen clinique et de l’IRM.
•
•Absence de maladie métastatique à la radiographie thora-
cique ou à l’IRM ou à la tomodensitométrie abdomino-pel-
vienne initiale ; absence d’envahissement des ganglion(s) para-
aortique(s).
•
•Traitement fondé sur une radiothérapie externe pelvienne
(45 Gy) associée à une chimiothérapie concomitante (cispla-
tine 40/mg/m2/semaine) suivie d’une curiethérapie utérovagi-
nale (15 Gy) ;
•
•Toutes les patientes ont bénéficié au moins d’une hystérecto-
mie extra-fasciale ; la radicalité de l’exérèse paramétriale a été
classée selon la classification de Piver (2).
•
•Présence à la fin de la radiothérapie d’une tumeur cervicale
résiduelle macroscopique mesurant au moins 2 cm (évaluée au
moins 6 semaines après la fin de la curiethérapie) et confirmée
lors de l’analyse histologique.
Les patientes ont été exclues de cette série pour les raisons sui-
vantes :
•
•Autres sous-types histologiques (carcinome à petites cel-
lules, mélanome ou sarcome).
•
• Absence d’IRM initiale.
•
•Délivrance d’une radiothérapie externe à une dose inférieure
à 45 Gy et/ou associée à du cisplatine à une dose différente de
40/mg/m2/semaine et/ou chimiothérapie concomitante asso-
ciant deux produits et/ou CRT au niveau de la zone pelvienne
et para-aortique.
•
• Absence de chirurgie pelvienne.
•
•Absence de tumeur cervicale résiduelle ou présence d’une
tumeur résiduelle minime (< 1 cm) lors de l’analyse histolo-
gique ou présence d’une maladie résiduelle sous forme de gan-
glion(s) lymphatique(s) métastatique(s) sans tumeur résiduelle
au niveau du col.
Les caractéristiques des patientes, les complications et les réci-
dives ont été étudiées. Les complications ont été classées selon
le glossaire franco-italien (3). Les courbes de survie ont été
déterminées à l’aide de la méthode de Kaplan-Meier.
DOSSIER
Chirurgie totale dans le cancer du col avec reliquat
tumorale résiduel après radio-chimiothérapie
●E. Azria (1), C. Haie-Meder (2), Y. Zafrani (1), P. Pautier (3), C. Lhommé (3), P. Duvillard (4), D. Castaigne (1), P. Morice (1)
Completion surgery in bulky cervical cancer
1. Service de chirurgie. 2. Service de radiothérapie. 3. Service d’oncologie
médicale. 4. Service d’anatomopathologie, institut Gustave-Roussy, 39, rue
Camille-Desmoulins, 94805 Villejuif.
L

34
DOSSIER
La Lettre du Gynécologue - n° 313 - juin 2006
RÉSULTATS
Douze patientes présentaient un reliquat tumoral cervical résiduel
volumineux à la fin de la CRT. Une patiente souffrait d’une car-
cinomatose péritonéale découverte lors de la chirurgie totale
(l’hystérectomie n’a donc pas été pratiquée). Une autre patiente a
subi l’intervention chirurgicale hors de notre hôpital et les infor-
mations complètes sur l’intervention chirurgicale, les résultats
histologiques et l’évolution postopératoire n’étaient pas dispo-
nibles. Des données complètes incluant les sept critères, précé-
demment décrits dans le chapitre “Patientes et méthodes”, étaient
disponibles pour seulement 10 patientes.
Les caractéristiques de ces 10 patientes sont rapportées dans le
tableau p. 35. L’âge médian était de 49 ans (extrêmes : 28-73).
Six des 10 patientes étaient ménopausées au moment du diagnos-
tic. La taille médiane de la tumeur était de 6 cm (de 4 à 9 cm). Le
diagnostic histologique était un carcinome épidermoïde dans 8 cas
et un adénocarcinome cervical dans 2 cas (patientes n°1 et 10).
Selon la classification FIGO, 2 patientes avaient une tumeur de
stade IIA et 8 de stade IIB. Le statut ganglionnaire initial a été
déterminé par IRM ou tomodensitométries (scanner) pelvienne
et abdominale. Chez cinq patientes, les ganglions pelviens ont
été considérés comme suspects avant traitement et 2 avaient de
petits ganglions para-aortiques inférieurs à 1 cm.
Concernant la chimio-radiothérapie, le nombre médian de
séances de radiothérapie externe a été de 24 et la durée totale
médiane de la radiothérapie externe a été de 36 jours. Deux
patientes ont reçu une radiothérapie latéro-pelvienne complé-
mentaire à une dose de 8 et 10 Gy en raison d’un envahisse-
ment des ganglions.
L’intervention chirurgicale a été pratiquée dans un intervalle
médian de 49 jours (extrêmes : 42-64) après la fin de la curie-
thérapie. Trois patientes ont eu une hystérectomie extra-fas-
ciale (patientes n° 2, 3 et 9), 6 une hystérectomie radicale de
type II (patientes n°1, 5, 6, 7, 8 et 10) et une exentération pel-
vienne totale (avec anastomose termino-terminale/patiente
n° 4). Huit patientes ont bénéficié d’une lymphadénectomie
pelvienne et 8 d’une lymphadénectomie para-aortique selon
une procédure précédemment décrite (4).
Toutes les patientes présentaient une maladie cervicale rési-
duelle > 2 cm. Toutes les patientes sauf une avaient des
marges chirurgicales négatives. La patiente chez laquelle
l’exérèse avait été incomplète a subi une hystérectomie radi-
cale de type II avec lymphadénectomie pelvienne et para-aor-
tique. Il y avait envahissement des marges vaginales lors de
l’exérèse. Cinq patientes présentaient au moins un ganglion
métastatique. Quatre patientes avaient un envahissement gan-
glionnaire pelvien (parmi elles, 1 seul ganglion positif a été
localisé dans le groupe iliaque externe). Un envahissement
ganglionnaire para-aortique était présent chez quatre patientes
(parmi elles, 1 présentait un envahissement isolé dans cette
région). Chez deux d’entre elles, de petits ganglions (< 1 cm)
existaient dans la région para-aortique lors de l’IRM ou la
tomodensitométrie initiale. Ainsi, chez trois patientes, on
notait un envahissement ganglionnaire dans les régions pel-
vienne et para-aortique. Parmi les patientes ayant des méta-
stases au niveau des ganglions lymphatiques, une rupture cap-
sulaire a été identifiée dans 4 cas. Le nombre de ganglions
positifs chez les patientes ayant un envahissement ganglion-
naire para-aortique a été le suivant : 4 sur 10 réséqués, 24 sur
31 réséqués, 4 sur 5 réséqués et 7 sur 10 réséqués. Un envahis-
sement de l’espace lymphatique et vasculaire a été observé
chez 6 patientes. Dans tous les cas, la cytologie péritonéale n’a
pas mis en évidence de cellules malignes.
Aucune des patientes ayant un envahissement ganglionnaire et
ayant eu un curage ganglionnaire para-aortique complet n’a eu
de radiothérapie para-aortique postopératoire (afin de réduire
le risque de complications intestinales), mais 3 patientes ont
reçu une chimiothérapie adjuvante à base de platine.
Au total, 14 complications de grade 2 ou 3 (selon le glossaire
franco-italien) ont été observées chez 7 patientes. Nous avons
documenté 4 complications de grade 3 (2 fistules urétérales
nécessitant un stent permanent, 1 embolie pulmonaire sévère
et 1 fistule rectovaginale nécessitant une colostomie définitive
chez la patiente ayant subi une exentération pelvienne) et 9
complications de grade 2 (2 drainages de lymphocèles, 1 phlé-
bite iliaque, 4 sténoses urétérales nécessitant la pose d’un stent
temporaire ou une intervention chirurgicale, 1 rétention vési-
cale nécessitant un sondage et 1 incontinence vésicale).
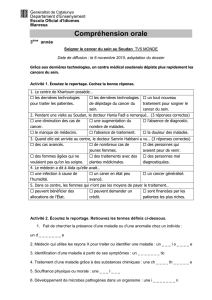
La durée médiane du suivi après chirurgie a été de 22 mois
(extrêmes : 1-37). Une patiente a été perdue de vue 1 mois
après l’intervention chirurgicale. La figure ci-dessus présente
la courbe de survie. Il y a eu récidive chez 7 patientes, princi-
palement sous forme métastatique (tableau p. 35). Une seule
patiente (la seule ayant un envahissement des marges) a pré-
senté une récidive pelvienne avec envahissement massif du
vagin, de la vessie et des parois pelviennes latérales, 6 mois
après l’intervention chirurgicale. Le délai médian entre chirur-
gie et récidive a été de 16 mois (extrêmes : 6-32).
Parmi les quatre patientes ayant une récidive localisée, au
moins dans le groupe présentant un envahissement ganglion-
naire para-aortique, toutes ont subi une lymphadénectomie à
ce niveau : l’examen histologique a révélé des ganglions lym-
phatiques positifs avec rupture capsulaire (trois d’entre elles
ont eu une chimiothérapie après l’intervention chirurgicale).
Quatre patientes ont succombé à leur maladie. Le délai médian
entre le diagnostic de la récidive et la date du décès a été de 6 mois
(extrêmes : 2-14). La survie médiane sans récidive a été de
18 mois (extrêmes : 6-34). La survie globale médiane a été de
24 mois (extrêmes : 9-37). Deux patientes seulement sont
vivantes sans récidive 27 et 19 mois après la fin du traitement.
Figure. Kaplan-Meier : survie indemne de récidive.
Mois
Survie

35
DOSSIER
La Lettre du Gynécologue - n° 313 - juin 2006
DISCUSSION
L’association d’une chimiothérapie concomitante à la radio-
thérapie externe permet d’obtenir un taux de survie sans réci-
dive supérieur de 16% à celui observé avec un traitement fai-
sant appel à la seule radiothérapie externe, en particulier chez
les patientes ayant un cancer du col de stade IB2 ou II (5). Les
taux de survie globale et de survie sans récidive sont améliorés
avec un nombre moindre de récidives locales et à distance (5).
La radiothérapie associée à une chimiothérapie à base de cis-
platine a été comparée à la radiothérapie seule dans plusieurs
études importantes récentes (6-8). Le traitement de référence
lors d’une chimiothérapie concomitante associée à la radiothé-
rapie est le cisplatine (9, 10). Désormais, la radiothérapie
externe associée à une chimiothérapie concomitante (cisplatine
40 mg/m2par semaine) est donc le traitement de référence du
cancer du col supérieur à 4 cm.
La justification d’une chirurgie pelvienne chez les patientes
traitées par radiothérapie exclusive fait toujours l’objet de
nombreux débats. Plusieurs analyses rétrospectives ont com-
paré des patientes ayant eu une hystérectomie ou n’ayant eu
aucune chirurgie pelvienne après radiothérapie (sans chimio-
thérapie concomitante). Lors de deux de ces études, les résul-
tats de survie ont été meilleurs chez les patientes ayant bénéfi-
cié d’une intervention chirurgicale après radiothérapie (11,
12). D’autres auteurs n’ont cependant pas retrouvé de tels
résultats (13-15). Dans notre pays, la chirurgie pelvienne de
complément est traditionnellement associée à la radiothérapie
externe (RTE) chez les patientes ayant un cancer du col de
stade IB2 et II (16-19). Les résultats des études portant sur ces
procédures classiques semblent intéressants en termes de sur-
vie. Un seul essai randomisé (achevé il y a 10 ans) vient d’être
récemment publié : il compare des patientes traitées par radio-
thérapie externe initiale et ensuite randomisées en deux bras :
un groupe bénéficiant d’une hystérectomie totale et l’autre
sans hystérectomie (20). Cette étude ne semble pas mettre en
évidence de bénéfice en termes de survie globale. Néanmoins,
une tendance à une augmentation de la survie sans récidive a
été notée chez les patientes ayant subi une hystérectomie (62
contre 53% à 5 ans, p = 0,09) (20).
Les avantages potentiels d’une hystérectomie après radiothéra-
pie externe sont doubles :
– Toute tumeur résiduelle éventuelle peut être réséquée dans
l’espoir d’améliorer ainsi la survie sans récidive.
– Le statut ganglionnaire peut être correctement évalué, ce qui
permet d’administrer un traitement adjuvant chez les patientes
ayant un envahissement ganglionnaire.
Concernant le premier point (exérèse d’une tumeur résiduelle
potentielle et amélioration de la survie), trois types de
patientes doivent être distingués après chimio-radiothérapie :
patientes sans tumeur résiduelle à la fin de la radiothérapie,
patientes ayant un petit reliquat tumoral résiduel (tumeur < 1 cm
ou groupes isolés de cellules tumorales dans des tissus partiel-
lement stérilisés) et patientes ayant de gros reliquats résiduels
(> 2 cm). Aucune étude randomisée n’a évalué quel bénéfice
apportait l’hystérectomie après chimio-radiothérapie. Lors de
l’étude randomisée portant sur la chimio-radiothérapie
conduite par Keys et al., une hystérectomie a été pratiquée
dans les deux groupes de traitement (8). Le taux de reliquat
tumoral résiduel après chimio-radiothérapie a été plus faible
chez les patientes soumises à une chimio-radiothérapie que
chez celles traitées par radiothérapie externe (48 % contre
59% ; p = 0,04) (8). Lors d’un essai rétrospectif français por-
tant sur 193 patientes soumises à différents protocoles de chi-
mio-radiothérapie suivis d’une chirurgie pelvienne, le pourcen-
tage de reliquat tumoral résiduel dans le cancer du col de stade
IB2 et II a été respectivement de 56 et 58% (21). Dans le cas
des patientes sans maladie résiduelle macroscopique confirmée
par l’examen clinique et l’IRM (8 semaines après la fin de la
CRT), un essai randomisé est actuellement en cours en France
afin d’évaluer l’impact de l’hystérectomie. Les patientes dont
le reliquat tumoral résiduel est de très petite taille (< 1 cm) se
trouvent probablement dans une situation similaire à celle des
patientes sans tumeur résiduelle ; si l’intervention chirurgicale
avait été pratiquée quelques semaines plus tard, ce résidu
aurait été totalement stérilisé par la chimio-radiothérapie.
La situation est totalement différente pour les patientes ayant
un gros reliquat tumoral résiduel. En principe, la chirurgie est
la seule manière d’augmenter la survie de ces patientes, en
réséquant le reliquat tumoral résiduel volumineux que la CRT
n’avait pas réussi à éradiquer. Cette étude porte sur un faible
nombre de patientes, elle est néanmoins originale. En effet, à
notre connaissance, la littérature ne comporte aucune donnée
sur les résultats de la chirurgie pelvienne chez des patientes
Tableau. Caractéristiques des 10 patientes.
Caractéristiques initiales Résultats anatomo-pathologiques Morbidités Intervalle** Récidives
Patient Âge Taille Ganglions Marges Statut LVSI* postopératoires Localisation Évolution***
de la tumeur
1 41 80 N+ Saines LVSI- Phlébite/sténose urétrale 34 Plèvre Décès à 36 mois
2 52 50 N+ Saines LVSI+ Sténose urétrale 18 Para-aortique APD à 37 mois
3 57 50 N+ Saines LVSI+ 0 7 Para-aortique/foie Décès à 23 mois
4 28 50 N- Saines LVSI- Fistule anastomotique/ Non 0 En vie à 27 mois
rétention vésicale
5 73 40 N- Saines LVSI- Incontinence urinaire Non 0 En vie à 19 mois
6 46 60 N+ Saines LVSI- Sténose urétrale/fistules/ 6 Para-aortique Décès à 9 mois
7 42 90 N+ Saines LVSI+ embolie pulmonaire 19 Para-aortique/ Décès à 25 mois
foie/thoracique
8 41 60 N- Positives LVSI+ 0 6 Pelvienne APD à 9 mois
9 53 80 N- Saines LVSI+ Sténose urétrale/ 27 Carcinose APD à 30 mois
incontinence urinaire
10 56 50 N- Saines LVSI+ 0 Inconnu 0 LFU à 1 mois
* : envahissement espace lymphatique et vasculaire. ** : délai entre la fin du traitement et la récidive. *** : APD : en vie avec persistance de la maladie. LFU : Perdue de vue.

36
DOSSIER
La Lettre du Gynécologue - n° 313 - juin 2006
ayant un reliquat tumoral volumineux après CRT. Le faible
nombre de patientes reflète l’efficacité de la chimio-radiothé-
rapie dans le traitement des tumeurs cervicales. En fait, sur les
75 patientes revues pour la présente étude, 12 seulement
avaient un gros reliquat tumoral résiduel. En outre, lors de la
présente étude, nous avons sélectionné des patientes ayant été
soumises au même protocole de CRT afin d’en optimiser
l’homogénéité. Bien que “seulement” 10 cas soient rapportés
dans la présente étude, la population est très homogène. Nos
résultats en termes de survie sont particulièrement décevants,
même avec un suivi de durée brève (suivi médian de 22 mois).
Sur les 9 patientes suivies, 2 seulement sont en vie sans réci-
dive. Ces résultats conduisent à s’interroger sur le bénéfice
réel de l’hystérectomie totale dans ce groupe de patientes ayant
des masses tumorales résiduelles volumineuses. En revanche,
il est intéressant de noter que la seule récidive pelvienne rap-
portée dans la présente étude ait été observée chez la patiente
dont les marges chirurgicales n’étaient pas saines. En outre, le
délai écoulé entre l’hystérectomie et la récidive a été de 16
mois. La patiente n’a donc pas souffert de symptômes pelviens
pénibles dus à une dissémination tumorale locale au cours de
cette période. Nous savons que lorsqu’une tumeur pelvienne
(récidive) n’est pas réséquée, elle se dissémine localement
avec des symptômes qui ont des effets désastreux sur la qualité
de vie de la patiente (leucorrhées nauséabondes, fistules recto-
vaginales ou fistules vésicovaginales). Ces deux points pour-
raient constituer des arguments puissants en faveur de l’hysté-
rectomie, même si son impact sur la survie sans récidives est
faible.
Existe-t-il un sous-groupe de patientes ayant un reliquat tumo-
ral résiduel volumineux dans lequel l’hystérectomie serait utile
? Lors de la présente étude, nous avons observé un taux élevé
de dissémination extra-cervicale : 1 patiente présentait une
tumeur péritonéale découverte au cours de la laparotomie
exploratrice et le taux d’envahissement ganglionnaire pelvien
et/ou para-aortique est élevé (50 %). Toutes ces patientes
avaient eu une IRM préopératoire et aucune ne présentait de
masses ganglionnaires volumineuses suspectes dans la région
para-aortique (2 étaient cependant porteuses de petits gan-
glions para-aortiques). La taille des ganglions para-aortiques
positifs était inférieure à 1 cm chez toutes les patientes mais
toutes ont rechuté. Plusieurs publications antérieures suggèrent
que l’exérèse de ganglions positifs a un intérêt thérapeutique
(22-25). Après radio-chimiothérapie pelvienne première, cette
hypothèse est plus discutable. En effet, la lymphadénectomie
n’a pas eu d’intérêt thérapeutique dans notre série de patientes
ayant des masses tumorales résiduelles volumineuses au
niveau du col : ainsi toutes les patientes ayant un envahisse-
ment ganglionnaire ont rechuté. Néanmoins, si nous analysons
la population de patientes sans envahissement ganglionnaire et
à marges saines (3 patientes) qui ont été suivies, 2 sont en vie
sans récidive. En termes de survie globale et de survie sans
récidive, la chirurgie pelvienne pourrait donc avoir un intérêt
chez des patientes sans tumeurs extra-cervicales. Un bilan
radiologique complet (IRM abdomino-pelvienne, radiogra-
phies thoraciques ± TDM) est nécessaire pour sélectionner ces
patientes et exclure celles ayant des métastases à distance.
L’imagerie PET/CT a été ajoutée à notre bilan systématique
afin de mieux sélectionner les candidates éventuelles à une
chirurgie de rattrapage. Un article récent suggère que l’image-
rie PET/CT permet de détecter de manière assez fiable une
maladie à distance (26). Si la PET/CT ne met pas en évidence
de maladie extra-pelvienne, une exploration laparoscopique
doit être pratiquée au début de l’intervention chirurgicale afin
d’éviter toute laparotomie inutile chez les patientes ayant une
maladie péritonéale.
L’évaluation des résultats de l’hystérectomie chez les patientes
ayant un gros reliquat résiduel serait incomplète si l’on n’abordait
pas un point important, à savoir le taux de complications. Weems
et al. et Mendenhall et al. ont rapporté précédemment que la chi-
rurgie augmente l’incidence des complications sévères chez les
patientes traitées initialement par radiothérapie externe (14, 15).
Par ailleurs, Thoms et al. et Galion et al., n’ont observé aucune
différence quant à l’incidence des complications sévères entre les
patientes ayant ou non eu une intervention chirurgicale (11, 12).
Lors d’une précédente étude conduite dans deux centres sur la
morbidité due à l’hystérectomie radicale après radiothérapie
externe pour cancer du col de stade IB2 ou II, le taux de morbidité
majeure a pratiquement atteint 25% (27). Ce taux n’a pas été dif-
férent selon les deux centres, mais il a été corrélé à la radicalité de
la chirurgie (chirurgie de type III de Piver). Nos résultats confir-
ment le taux élevé des complications de la chirurgie pelvienne
après chimio-radiothérapie. Lors de la précédente étude de Keys
et al., le taux des complications de grade 2 ou 3 après hystérecto-
mie extra-fasciale a été pratiquement de 35% (20). Dans la pré-
sente étude, ce taux est très élevé. Le taux de complications d’une
chirurgie radicale est probablement plus élevé après chimio-radio-
thérapie qu’après radiothérapie externe. Les complications les
plus fréquentes ont été les complications urétérales et ont été liées
à la dissection du paramètre. Cependant, dans la présente série,
aucune des patientes n’a eu d’hystérectomie radicale de type III.
Chez les patientes ayant un reliquat tumoral résiduel volumineux,
il est très difficile de pratiquer une hystérectomie extra-fasciale
simple si le principal objectif est d’obtenir des marges saines. La
dissection de la partie proximale du paramètre est donc impéra-
tive pour garantir la qualité des marges latérales et mieux repé-
rer les uretères. Le taux élevé de complications est le prix à
payer pour une telle intervention.
Notre série confirme que le taux d’envahissement ganglion-
naire est élevé chez les patientes dont le reliquat tumoral cervi-
cal résiduel est volumineux après chimio-radiothérapie (CRT).
En outre, les patientes ont présenté un taux de complications
élevé (70%) après chirurgie pelvienne. Deux patientes seule-
ment sont en vie et sans récidive. Les résultats de la chirurgie
sont donc décevants. Cette chirurgie totale devrait probable-
ment faire l’objet d’une évaluation lors d’un essai randomisé,
mais le pourcentage de patientes avec un gros reliquat tumoral
résiduel étant faible après CRT suivie d’une curiethérapie, un
tel essai est probablement irréalisable. Une solution consiste-
rait à inclure ce sous-groupe de patientes dans l’étude rando-
misée en cours dont l’objectif est d’évaluer l’intérêt de l’hysté-
rectomie chez les patientes sans tumeur résiduelle
macroscopique à la fin de la chimio-radiothérapie. ■
Remerciements : Les auteurs remercient Lorna Saint Ange pour son assis-
tance à la préparation de cet article.

37
DOSSIER
RÉFÉRENCES BIBLIOGRAPHIQUES
1. Parkin DM. Global cancer statistics in the year 2000. Lancet Oncol 2001;2:533-
43.
2. Piver MS, Rutledge F, Smith JP. Five classes of extended hysterectomy for women
with cervical cancer. Obstet Gynecol 1974; 44:265-72.
3. Chassagne D, Sismondi P, Horiot JC, Sinistero G, Bey P, Zola P et al. A glossary
for reporting complications of treatment in gynecological cancers. Radiother Oncol
1993;26:195-202.
4. Michel G, Morice P, Castaigne D, Leblanc M, Rey A, Duvillard P. Lymphatic
spread of stage IB/II cervical carcinoma: anatomy and surgical implications. Obstet
Gynecol 1998;91:360-3.
5. Green JA, Kirwan JM, Tierney JF, Symonds P, Fresco L, Collingwood et al.
Survival and recurrence after concomitant chemotherapy and radiotherapy for can-
cer of the uterine cervix : a systematic review and meta-analysis. Lancet
2001;358:781-6.
6. Morris M, Eifel PJ, Lu J, Grigsby PW, Levenback C, Stevens RE et al. Pelvic
radiation with concurrent chemotherapy compared with pelvic and para-aortic
radiation for high-risk cervical cancer. N Engl J Med 1999;340 1137-43.
7. Peters WA 3rd, Liu PY, Barrett RJ 2nd, Stock RJ, Monk BJ, Berek JS et al.
Concurrent chemotherapy and pelvic radiation therapy compared with pelvic radia-
tion therapy alone as adjuvant treatment after radical surgery in high-risk early-
stage cancer of the cervix. J Clin Oncol 2000;18:1606-13.
8. Keys HM, Bundy BN, Stehman FB, Muderspach LI, Chafe WE, Stuggs III CL et al.
Cisplatin, radiation and adjuvant hysterectomy compared with radiation and adju-
vant hysterectomy for bulky stage Ib cervical carcinoma. N Engl J Med
1999;341:708.
9. Rose PG, Bundy BN, Watkins EB, Thigpen JT, Deppe G, Maiman MA et al.
Concurrent cisplatin-based radiotherapy and chemotherapy for locally advanced
cervical cancer. N Engl J Med 1999;340:1144-53.
10. Whitney CW, Sause W, Bundy BN, Malfetano JH, Hhanningan EV, Fowler WC
Jr et al. Randomized comparaison of fluorouracil plus cisplatin versus hydroxyurea
as an adjunct to radiation therapy in stage II-IVA carcinoma of the cervix with nega-
tive para-aortic lymph nodes: a Gynecologic Oncology Group and Southwest
Oncology Group study. J Clin Oncol 1999;17:1339-48.
11. Gallion HH, Van Nagell JR, Donaldson ES, Hanson MB, Powell DE, Maruyama
Y et al. Combined radiation therapy and extrafacial hysterectomy in the treatment of
stage IB barrel-shaped cervical cancer. Cancer 1985;56:262-5.
12. Thoms WW, Eifel P, Smith T, Morris M, Delclos L, Wharton JT, Oswald MJ.
Bulky endocervical carcinoma: a 23-year experience. Int J Radiat Oncology Biol
Phys 1992;23:491-9.
13. Perez CA, Kao MS. Radiation therapy alone or combined with surgery in the
treatment of barrel-shaped carcinoma of the uterine cervix (stages IB, IIA, IIB). Int J
Radiat Oncology Biol Phys 1985;11:1903-9.
14. Weems DH, Mendenhall WM, Bova FJ, Marcus RB, Morgan LS, Million RR.
Carcinoma of the intact uterine cervix, stage IB-IIA-B, > 6 cm in diameter: irradia-
tion alone vs preoperative irradiation and surgery. Int J Radiat Oncology Biol Phys
1985;11:1911-4.
15. Mendenhall WM, McCarty PJ, Morgan LS, Chafe WE, Million RR. Stage IB or
IIA-B carcinoma of the intact uterine cervix ≥6 cm in diameter: is adjuvant extrafa-
cial hysterectomy beneficial? Int J Radiat Oncology Biol Phys 1991;21:899-904.
16. Touboul E, Lefranc JP, Blondon J, Ozsahin M, Roche B, Mauban S et al.
Preoperative radiation therapy and surgery in the treatment of “bulky” squamous
cell carcinoma of the uterine cervix (stage IB, IIA and IIB operable tumors).
Radiother Oncol 1992;24:32-40.
17. Bernard A, Touboul E, Lefranc JP, Deniaud-Alexandre E, Genestie C, Uzan S et
al. Epidermoid carcinoma of the uterine cervix at operable bulky stage I and II trea-
ted with combined primary radiation therapy and surgery. Cancer Radiother 2002;
6:85-98.
18. Resbeut M, Cowen D, Viens P, Noirclerc M, Perez T, Gouvernet J et al.
Concomitant chemoradiation prior to surgery in the treatment of advanced cervical
carcinoma. Gynecol Oncol 1994;54:68-75.
19. Morice P, Haie-Meder C, Rey A, Pautier P, Lhommé C, Gerbaulet A et al.
Radiotherapy and radical surgery for patients with bulky stage IB and II cervical car-
cinoma. Int J Gynecol Cancer 2000;10:239-46.
20. Keys HM, Bundy BN, Stehman FB, Okagaki T, Gallup DG, Burnett AF et
al.Radiation therapy with or without extrafascial hysterectomy for bulky stage IB cer-
vical carcinoma: a randomized trial of the Gynecologic Oncology Group. Gynecol
Oncol 2003;89:343-53.
21. Classe JM, Morice P, Rodier JF, Rauch P, Lasry S, Houvenaeghel G.
Pathological evaluation of pelvic radiotherapy with concurrent cisplatin-based che-
motherapy followed by surgery in treatment of locally advanced cervical cancer: a
retrospective multicentric experience of French Federation of Cancer Centers. EJSO
2002;28:300.
22. Hacker NF, Wain GV, Nicklin JL. Resection of bulky positive lymph nodes in
patients with cervical carcinoma. Int J Gynecol Cancer 1995;5:250-6.
23. Downey GO, Potish RA, Adcock LL, Prem KA, Twiggs LB. Pretreatment surgical
staging in cervical carcinoma: therapeutic efficacy of pelvic lymph node resection.
Am J Obstet Gynecol 1989;160:1055-61.
24. Cosin JA, Fowler JM, Chen MD, Paley PJ, Carson LF, Twiggs LB. Pretreatment
surgical staging of patients with cervical carcinoma. The case for lymph node debul-
king. Cancer 1998;82:2241-8.
25. Morice P, Castaigne D, Pautier P, Rey A, Haie-Meder C, Leblanc M, Duvillard
P. Interest of pelvic and para-aortic lymphadenectomy in patients with stage IB and
II cervical carcinoma. Gynecol Oncol 1999;73:106-10.
26. Lai CH, Huang KG, See LC, Yen TC, Tsai CS, Chang TC, et al. Restaging of
recurrent cervical carcinoma with dual-phase [18F]fluoro-2-deoxy-D-glucose posi-
tron emission tomography. Cancer 2004;100:544-52.
27. Morice P, Le Bouedec G, Pomel C, Haie-Meder C, Achard JL, Lhommé C et al.
Complications of primary external radiation therapy followed by radical hysterec-
tomy for bulky stage IB and II cervical cancer. 2001;37,Suppl.6:1232.
La Lettre du Gynécologue - n° 313 - juin 2006
Communiqué AFACS (Association française pour l’après cancer du sein)
L’incidence du cancer du sein est en pleine expansion : le nombre de cas a quasiment doublé en France depuis 25 ans. En revanche, grâce d’une part,
aux progrès de dépistage et d’autre part, à l’oncologie moderne, le nombre de femmes ayant eu un cancer du sein encore en vie suit une irrésistible
courbe exponentielle avec plus de 90 % de rémissions complètes obtenues après traitement de la phase aiguë : aujourd’hui dans notre pays, plus de
400 000 femmes sont donc concernées par cet “après cancer du sein”. L’objectif premier est certes carcinologique : dépister les rechutes locales, les
cancers homolatéraux et les métastases, de même qu’évaluer les traitements institués après la phase aiguë. Mais, à juste titre, ces femmes sont aussi
de plus en plus exigeantes envers leurs médecins sur des domaines variés regroupés sous le terme : “qualité de vie” tels que la gestion des effets
secondaires des traitements institués, l’évaluation du risque cardiovasculaire, la sexualité, la possibilité d’éventuelle grossesse, la contraception,
l’éventuelle reconstruction mammaire, le contrôle du poids, le maintien de leur masse osseuse et de la peau, la réinsertion conjugale, professionnelle
et sociale, le soutien moral nécessaire, etc. Elles entendent mener une bonne qualité de vie, ce qui nécessite d’avoir une surveillance et un suivi adap-
tés. Nos collègues oncologues sont de plus en plus sollicités pour cette surveillance de “l’après cancer” et par la même gênés dans leurs missions
principales : la mise en œuvre thérapeutique face à la tumeur et la gestion des récidives et métastases. Les consultations de suivi, parce qu’elles sont
de plus en plus nombreuses et que les femmes souhaitent bien plus que leur suivi oncologique strict, sont une charge de travail supplémentaire, sou-
vent “asphyxiante” au quotidien et les médecins manquent. C’est sur ce constat que la décision de créer une société savante spécifiquement consa-
crée au suivi du cancer du sein dans tous ses aspects a été prise. L’objectif de l’AFACS est “d’optimiser le suivi des femmes atteintes de cancer du
sein, en dehors de la phase aiguë, en assurant la surveillance, en veillant par tout les moyens à leur qualité de vie et en encourageant la recherche et la
diffusion des connaissances sur le sujet”. L’AFACS entend accueillir tous les médecins tant gynécologues, généralistes que tout autre
spécialité, intéressés au suivi et à la surveillance de ces femmes dans cette dimension “interniste”, afin qu’ils deviennent des acteurs
efficaces de cette surveillance aux côtés des oncologues. L’AFACS n’entend pas concurrencer les oncologues dans leurs actions spé-
cifiques, mais venir en soutien en des domaines variés liés à la qualité de vie de ces femmes.
AFACS : 169, bd Haussmann, 758008 Paris. E-mail : [email protected]
1
/
5
100%