E Métastases hépatiques de cancer colo-rectal : stratégie médico-chirurgicale

CAS CLInIquE
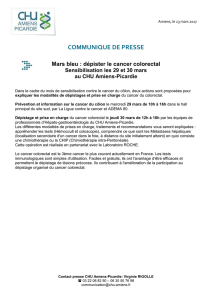
Figure 1. Métastases hépatiques de cancer colo-rectal
avant 7 cures de FOLFIRI-bévacizumab.
314 | La Lettre du Cancérologue • Vol. XVIII - n° 6 - juin 2009
Métastases hépatiques
de cancer colo-rectal :
stratégie médico-chirurgicale
Colorectal liver metastases: medical-surgical strategy
D. Malka*, A. Sa Cunha**
* Département de médecine, institut Gustave-Roussy, Villejuif.
** Service de chirurgie, groupe hospitalier Sud, Bordeaux.
E
n cas de métastases hépatiques de cancer colo-rectal
(MHCR) résécables d’emblée (dans 10 à 20 % des cas),
une chimiothérapie périopératoire par FOLFOX-4
permet de diminuer les récidives (1).
En cas de MHCR non résécables (80 à 90 % des cas), environ
15 % – mais ce chiffre croît – peuvent le devenir en cas de
réponse objective tumorale à une chimiothérapie.
Observation
Une colectomie gauche était effectuée en urgence pour cancer
du côlon gauche perforé chez un homme de 65 ans sans anté-
cédent. L’exploration peropératoire et la tomodensitométrie
thoraco- abdomino-pelvienne postopératoire montraient l’ab-
sence de carcinose péritonéale et des MHCR bilatérales isolées
(figure 1), considérées comme non résécables en réunion
de concertation pluridisciplinaire oncologique (RCPO). Une
combinaison FOLFIRI-bévacizumab était instaurée. À l’issue
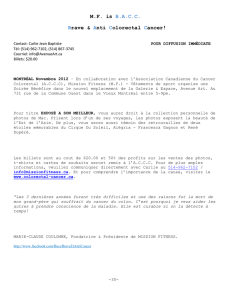
de 7 cures, une réponse objective était observée (figure 2).
Il était alors décidé d’un premier temps chirurgical (tumo-
rectomie gauche avec radiofréquence de deux MHCR du
segment IV suivie d’une embolisation portale droite), puis
d’un second temps chirurgical (hépatectomie droite élargie
Mots-clés
Cancer colo-rectal – Chimiothérapie – Chirurgie
Keywords
Colorectal cancer
–
Chemotherapy
–
Surgery

CAS CLInIquE
Figure 2. Métastases hépatiques de cancer colo-rectal après
7 cures de FOLFIRI-bévacizumab.
La Lettre du Cancérologue • Vol. XVIII - n° 6 - juin 2009 | 315
au segment I) 3 mois plus tard, la chimiothérapie étant pour-
suivie entre les deux temps opératoires (avec arrêt du FOLFIRI
et du bévacizumab respectivement 4 et 6 semaines avant),
puis au décours. Un an après l’hépatectomie, le patient était
indemne de récidive.
Discussion
La chimiothérapie “d’induction” idéale doit permettre d’ob-
tenir un taux de réponse objective maximal. G. Folprecht et
al. ont en effet montré chez des patients “non sélectionnés”
inclus dans des essais de phase III que le taux de réponse
objective (31 à 59 %) et le taux de résécabilité secondaire des
MHCR (1 à 22 %) étaient corrélés de façon linéaire (r = 0,67,
p = 0,024), la corrélation étant maximale en cas de MHCR
isolées (r = 0,96, p = 0,002) [2]. Les bithérapies cytotoxiques
(fl uoropyrimidine + oxaliplatine ou irinotécan) donnent des
taux de réponse objective équivalents, de l’ordre de 50 % (3).
L’administration intra-artérielle hépatique de l’oxaliplatine
associée à un schéma LV5FU2 intraveineux (4) et les trithé-
rapies (FOLFIRINOX [5] ou FOLFOXIRI [6]) donnent des taux
de réponse objective égaux ou supérieurs à 60 %.
En l’absence de mutation tumorale du gène KRAS, l’addition
de cétuximab à une bithérapie cytotoxique permet d’atteindre
des taux de réponse objective équivalents (7, 8). En revanche,
cette addition est ineffi cace (7, 8), voire délétère, en cas de
mutation tumorale de KRAS (8).
À l’inverse, dans une analyse rétrospective de l’essai de
phase III de H.I. Hurwitz et al. (9), le bénéfi ce de l’addition du
bévacizumab à une bithérapie cytotoxique paraît indépen-
dant du statut KRAS, et chez les patients avec statut tumoral
KRAS sauvage, un taux de réponse objective de 60 % a été
observé.
L’équipe du MD Anderson Cancer Center a montré un bénéfi ce
de l’association du bévacizumab à un schéma FOLFOX en
termes de taux de réponse objective, de réponse histologique
et de résécabilité secondaire des MHCR (10, 11). La mauvaise
surprise causée par les essais PACCE (12) et CAIRO-2 [13]
(moindre effi cacité, toxicité supérieure) a fermé pour l’instant la
voie de la bithérapie ciblée (bévacizumab + anticorps anti-EGFR
de type cétuximab ou panitumumab) associée à une bithé-
rapie cytotoxique. Les premiers résultats d’essais de phase II de
trithérapie cytotoxique + cétuximab (14) ou bévacizumab (15)
sont prometteurs en termes de taux de réponse objective, mais
au prix d’une toxicité non négligeable, notamment digestive
(diarrhée) avec le cétuximab, ce qui a conduit à recommander
une dose moindre d’irinotécan (150 mg/m²) [14].
Par ailleurs, il est désormais acquis qu’un contrôle tumoral est
un préalable indispensable à toute chirurgie des MHCR, les
résultats à long terme chez les patients opérés en progression
tumorale étant médiocres (survie à 5 ans de 8 %) [16].
La chimiothérapie d’induction idéale doit aussi avoir une
morbidité faible. L’irinotécan et l’oxaliplatine exposent
à une surmorbidité après hépatectomie majeure (17), en
particulier en cas de chimiothérapie préopératoire récente
(< 4 semaines) [18] ou prolongée (plus de 6-8 cures) [10, 19].
Il faut donc obtenir rapidement une réponse objective suffi -
sante, la prolongation de la chimiothérapie au-delà de 8 cures
étant en règle générale peu effi cace (10).
L’administration de bévacizumab avant hépatectomie, même
majeure, paraît sûre en termes de morbidité hépatique ou

CAS CLInIquE
316 | La Lettre du Cancérologue • Vol. XVIII - n° 6 - juin 2009
1. Nordlinger B, Sorbye H, Glimelius B et al. Perioperative
chemotherapy with FOLFOX4 and surgery versus surgery
alone for resectable liver metastases from colorectal
cancer (EORTC Intergroup trial 40983): a randomised
controlled trial. Lancet 2008;371:1007-16.
2. Folprecht G, Grothey A, Alberts S, Raab HR, Köhne CH.
Neoadjuvant treatment of unresectable colorectal liver
metastases: correlation between tumour response and
resection rates. Ann Oncol 2005;16:1311-9.
3. Tournigand C, André T, Achille E et al. FOLFIRI followed
by FOLFOX6 or the reverse sequence in advanced
colorectal cancer: a randomized GERCOR study. J Clin
Oncol 2004;22:229-37.
4. Ducreux M, Ychou M, Laplanche A et al. Hepatic arterial
oxaliplatin infusion plus intravenous chemotherapy in
colorectal cancer with inoperable hepatic metastases:
a trial of the gastrointestinal group of the Fédération
Nationale des Centres de Lutte Contre le Cancer. J Clin
Oncol 2005;23:4881-7.
5. Ychou M, Viret F, Kramar A et al. Tritherapy with
fl uorouracil/leucovorin, irinotecan and oxaliplatin
(FOLFIRINOX): a phase II study in colorectal cancer
patients with non-resectable liver metastases. Cancer
Chemother Pharmacol 2008;62:195-201.
6. Falcone A, Ricci S, Brunetti I et al. Phase III trial of
infusional fl uorouracil, leucovorin, oxaliplatin, and
irinotecan (FOLFOXIRI) compared with infusional
fl uorouracil, leucovorin and irinotecan (FOLFIRI) as
fi rst-line treatment for metastatic colorectal cancer:
the Gruppo Oncologico Nord Ovest. J Clin Oncol
2007;25:1670-6.
7. Van Cutsem E, Köhne CH, Hitre E et al. Cetuximab
and chemotherapy as initial treatment for metastatic
colorectal cancer. N Engl J Med 2009;360:1408-17.
8. Bokemeyer C, Bondarenko I, Hartmann JT et al. KRAS
status and effi cacy of fi rst-line treatment of patients
with metastatic colorectal cancer with FOLFOX with or
without cetuximab: the OPUS expe rience. J Clin Oncol
2008;26(Suppl. 15):abstract 4000.
9. Hurwitz HI, Yi J, Ince W, Novotny WF, Rosen O. The
clinical benefi t of bevacizumab in metastatic colorectal
cancer is independent of K-ras mutation status: analysis
of a phase III study of bevacizumab with chemotherapy
in previously untreated metastatic colorectal cancer.
Oncologist 2009;14:22-8.
10. Zorzi D, Kishi Y, Maru DM et al. Effect of extended
preoperative chemotherapy on pathologic response and
postoperative liver insuffi ciency after hepatic resection
for colorectal liver metastases. ASCO GastroIntestinal
Cancers Symposium 2009:abstract 295.
11. Blazer DG 3rd, Kishi Y, Maru DM et al. Pathologic
response to preoperative chemotherapy: a new outcome
end point after resection of hepatic colorectal metastases.
J Clin Oncol 2008;26:5344-51.
12. Hecht JR, Mitchell E, Chidiac T et al. A randomized phase IIIB
trial of chemotherapy, bevacizumab and panitumumab
compared with chemotherapy and bevacizumab alone for
metastatic colorectal cancer. J Clin Oncol 2009;27:672-80.
13. Tol J, Koopman M, Cats A et al. Chemotherapy,
bevacizumab and cetuximab in metastatic colorectal
cancer. N Engl J Med 2009;360:563-72.
14. Ychou M, Desseigne F, Thezenas S et al. Preliminary
results of a multicentre phase II trial evaluating cetuximab
in combination with FOLFIRINOX (LV5FU + irinotecan +
oxaliplatin) as fi rst-line treatment of metastatic colorectal
cancer (mCRC) patients. ASCO GastroIntestinal Cancers
Symposium 2009:abstract 450.
15. Falcone A, Masi G, Loupakis F et al. FOLFOXIRI
(irinotecan, oxaliplatin, and infusional 5FU/LV) in
combination with bevaci zumab in the fi rst-line treatment of
metastatic colorectal cancer: a phase II study by the GONO
group. J Clin Oncol 2008;26(Suppl. 15):abstract 4031.
16. Adam R, Pascal G, Castaing D et al. Tumor progression
while on chemotherapy: a contraindication to liver
resection for multiple colorectal metastases? Ann Surg
2004;240:1052-64.
17. Vauthey JN, Pawlik TM, Ribero D et al. Chemotherapy
regimen predicts steatohepatitis and an increase in 90-day
mortality after surgery for hepatic colorectal metastases.
J Clin Oncol 2006;24:2065-72.
18. Welsh FK, Tilney HS, Tekkis PP, John TG, Rees
M. Safe liver resection following chemotherapy for
colorectal metastases is a matter of timing. Br J Cancer
2007;96:1037-42.
19. Karoui M, Penna C, Amin-Hashem M et al. Infl uence
of preoperative chemotherapy on the risk of major
hepatectomy for colorectal liver metastases. Ann Surg
2006;243:1-7.
20. D’Angelica M, Kornprat P, Gonen M et al. Lack of evidence
for increased operative morbidity after hepatectomy with
perioperative use of bevacizumab: a matched case-control
study. Ann Surg Oncol 2007;14:759-65.
21. Kesmodel SB, Ellis LM, Lin E et al. Preoperative
bevacizumab does not signifi cantly increase postoperative
complication rates in patients undergoing hepatic surgery
for colorectal cancer liver metastases. J Clin Oncol 2008;
26:5254-60.
22. Reddy SK, Morse MA, Hurwitz HI et al. Addition
of bevacizumab to irinotecan- and oxaliplatin-based
preoperative chemotherapy regimens does not increase
morbidity after resection of colorectal liver metastases.
J Am Coll Surg 2008;206:96-106.
23. Cassidy J, Cunningham D, Berry SR et al. Surgery with
curative intent in patients with fi st-line chemotherapy +
bevacizumab for metastatic colorectal cancer: First BEAT
and NO 16966. J Clin Oncol 2008;26(Suppl. 15):abstract
4022.
24. Ribero D, Wang H, Donadon M et al. Bevacizumab
improves pathologic response and protects against
hepatic injury in patients treated with oxaliplatin-based
chemotherapy for colorectal liver metastases. Cancer
2007;110:2761-7.
25. Zorzi D, Chun YS, Madoff DC, Abdalla EK, Vauthey
JN. Chemotherapy with bevacizumab does not affect
liver regeneration after portal vein embolization in the
treatment of colorectal liver metastases. Ann Surg Oncol
2008;15:2765-72.
Références bibliographiques
générale tant dans les séries chirurgicales (20-22) que dans
les essais de phase III ou les grandes cohortes observation-
nelles totalisant plusieurs milliers de patients (23), pour peu
qu’un délai minimal de 5 à 8 semaines soit respecté entre la
dernière administration et la chirurgie.
Le bévacizumab paraît même diminuer l’incidence du syndrome
d’obstruction sinusoïdale induit par l’oxaliplatine (10, 24)
et, subséquemment, les besoins transfusionnels peropéra-
toires (22).
Enfin, le bévacizumab ne compromet pas l’hypertrophie
compensatrice de ce qu’il restera du foie restant après embo-
lisation portale (25).
Conclusion
L’évaluation initiale en RCPO des patients présentant des MHCR
est cruciale afi n d’identifi er les cas résécables d’emblée et, parmi
les cas non résécables, ceux qui peuvent le devenir après chimio-
thérapie d’induction optimale – c’est-à-dire une chimiothérapie
à la fois hautement et rapidement effi cace et peu morbide.
Cette évaluation initiale permet de défi nir une stratégie de
prise en charge médico-chirurgicale personnalisée (durée de
la chimiothérapie, délai chimiothérapie-chirurgie, radiofré-
quences, chirurgie en un ou deux temps, embolisation portale
si nécessaire), qu’il importera de réévaluer et, le cas échéant,
d’adapter à chaque étape du traitement. ■
1
/
3
100%