Caractéristiques et implications cliniques ESR1

1
Présenté par Laëtitia Augusto, le 24 Juin 2017
Sous la direction de Monsieur le Professeur Frédéric DI FIORE et Monsieur le
Docteur Florian CLATOT
Unité de Formation et de Recherche de médecine pharmacie
Université de ROUEN
Rapporteur : Pr Antoine Adenis, université de Lille
Mémoire pour l’obtention du diplôme d’études
spécialisées d’oncologie médicale
Caractéristiques et implications cliniques
de la détection des mutations circulantes
du gène ESR1 chez des patientes traitées
pour un cancer du sein métastatique en
progression sous anti-aromatase

2
Table des matières
I. GLOSSAIRE ..................................................................................................................................3
II. INTRODUCTION ...........................................................................................................................4
III. RATIONNEL DE L’ETUDE...........................................................................................................6
IV. MATERIEL ET METHODES ........................................................................................................8
a. Patients ...............................................................................................................................8
b. Echantillons sanguins ...........................................................................................................8
c. Détection par droplet digital Polymerase Chain Reaction (ddPCR) .......................................9
d. Seuil de positivité ................................................................................................................9
e. Analyse statistique ............................................................................................................ 10
V. RESULTATS ................................................................................................................................ 11
a. Caractéristiques et suivi des patientes ............................................................................... 11
b. Statut mutationnel à progression ...................................................................................... 11
c. Valeur pronostique ............................................................................................................ 12
d. Valeur prédictive des traitements ultérieurs à la progression sous AA ............................... 14
d.1 Traitement post progression par chimiothérapie ........................................................... 14
d.2 Traitement post progression par hormonothérapie ....................................................... 14
e. Cinétique ESR1 avant progression ...................................................................................... 15
f. Cinétique ESR1 après progression ...................................................................................... 16
VI. DISCUSSION .......................................................................................................................... 17
VII. CONCLUSION ......................................................................................................................... 20
VIII. BIBLIOGRAPHIE : ................................................................................................................... 21
IX. ANNEXES: .............................................................................................................................. 25

3
I. GLOSSAIRE
AA : Anti Aromatase
ADN : Acide DésoxyriboNucléique
ASCO : American Society of Clinical Oncology
CHB : Centre Henri Becquerel
cfDNA : ADN libre circulant
ctDNA : ADN tumoral circulant
dPCR : digital Polymerase Chain Reaction
ddPCR : droplet digital Polymerase Chain Reaction
ESR1 : Estrogen Receptor 1
FVA : Fraction Variant Allélique
HER2 : Human Epidermal growth factor Receptor 2
HR : Hazard Ratio
IC : Intervalle de Confiance
IRON : équIpe de Recherche en ONcologie
LBD : domaine de liaison au ligand
mESR1 : Mutation ESR1
NGS : Next Generation Sequencing
PI3K : PhosphoInositide 3-Kinase
RH : Récepteurs Hormonaux
RO : Récepteur Œstrogènes
RR : Risque Relatif
SBR : Scarff-Bloom-Richardson
SG : Survie Globale
SSR : Survie Sans Récidive
Tp : Temps à la progression sous AA
Tp-6 : 6mois avant progression sous AA
Tp-3 : 3mois avant progression sous AA
Tp+3 : 3mois après progression sous AA

4
II. INTRODUCTION
Le cancer du sein se situe au 1er rang des cancers incidents chez la femme. Ainsi,
54 062 nouveaux cas de cancer du sein ont été diagnostiqués en 2015 en France
métropolitaine(1). Environ 11 913 femmes en décèderaient faisant de ce cancer la
première cause de mortalité féminine par cancer en France (Projection Inca 2015).
On remarque, sur ces dernières années, une hausse du taux d’incidence
parallèlement à une diminution de la mortalité. Le dépistage organisé, une prise en
charge plus précoce ainsi que l’amélioration de la thérapeutique peuvent expliquer
au moins en partie cette évolution inverse. Il est important de distinguer les cancers
du sein localisés, des cancers du sein métastatiques. Ces derniers représentent 10%
des cas de cancer du sein au diagnostic, mais 20 à 30% des cancers initialement
localisés deviendront secondairement métastatiques.
Différents facteurs pronostiques du risque de rechute métastatique et du décès ont
été identifiés au plan clinique et histologique. Ainsi, la taille tumorale(2), l’atteinte
ganglionnaire ou non(3), l’âge de la patiente(4) et le caractère inflammatoire ou non
de la tumeur sont les principaux facteurs pronostiques cliniques du cancer du sein.
Sur le plan histologique, les principaux facteurs pronostiques sont le grade de Scarff,
Bloom et Richardson(5), la qualité des marges d’exérèse(6), la présence ou non
d’embole vasculaire(7) et le Ki67(8). L’amplification du gène HER2 présente dans 15
à 20% des cancers du sein constitue un critère de mauvais pronostique mais prédit
une réponse au traitement par anticorps monoclonaux anti-HER2(9). La présence de
récepteurs hormonaux (RH) à la surface des cellules tumorales est retrouvée dans
70% des cancers du sein et est un facteur de bon pronostique(10). Leur présence
conditionne la réponse à l’hormonothérapie et en fait un facteur prédictif majeur(11).
Le traitement par hormonothérapie représente un axe thérapeutique de choix chez
les patientes suivies pour un cancer du sein lors de la phase adjuvante d’un
traitement local, mais également lors de la phase métastatique dès la 1ère ligne(12).
Après la ménopause, la sécrétion d’hormones par les ovaires décline rapidement et
la principale source d’œstrogènes provient alors de la conversion périphérique des
androgènes d’origine surrénalienne (andostenedione et testostérone) par
l’aromatase présente dans le foie, le muscle, les follicules pileux, le tissu adipeux et
les cellules tumorales. Les inhibiteurs de l’aromatase (AA) permettent ainsi de
supprimer cette activité. Actuellement, le traitement par AA en première ligne du
cancer du sein avancé est associé à un taux de réponse global de 32%, une survie
sans progression (SSP) de 9,4 mois et une survie globale (SG) de 34 mois(13) et
constitue un traitement de référence. Cependant, malgré une bonne efficacité initiale,
l’émergence de résistances secondaires ou acquises est inéluctable et aboutit à une
progression tumorale. Cette hormonorésistance survient en moyenne 8 à 11 mois
après l’instauration du traitement et correspond à l’apparition de résistance en lien
avec la pression thérapeutique (14). En 1997, est mis en évidence pour la première
fois une mutation de novo située au niveau du gène codant les récepteurs aux
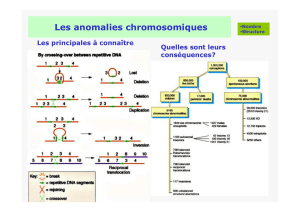
œstrogènes (RO) (15). Les RO appartiennent à la famille des récepteurs nucléaires
caractérisés par la segmentation en 5 régions communes nommées A/B, C, D, E et F
(Figure 1).

5
Ces régions participent à la formation des domaines fonctionnels suivants :
- le domaine N-terminal (région A et B) qui a pour principal rôle l’activation de la
transcription,
- le domaine de liaison à l'ADN ou DBD (région C) qui comme son nom l’indique
participe à la liaison à l’ADN et joue un rôle dans la dimérisation des
récepteurs,
- la région charnière (région D) qui a la capacité de changer de conformation
après fixation du ligand et ensuite permet au récepteur de migrer dans
le noyau cellulaire,
- la région C-terminale (région E et F) qui a pour rôle principal la fixation du
ligand ; on parle de domaine de liaison au ligand ou LBD.
Figure 1 : Structure des récepteurs aux œstrogènes
Des études plus récentes réalisées à partir de séquençage de tumeurs ont montré
que les mutations au niveau du gène codant le RO (Estrogen Receptor 1 ou ESR1),
rares sur les tumeurs primitives, pourraient expliquer des résistances secondaires à
l’hormonothérapie (16), ce d’autant que ces mutations affectent le LBD du gène
ESR1(17). En effet, plusieurs études indépendantes ont analysé des métastases de
patientes présentant un cancer du sein devenu hormonorésistant(17–19). Ces
études retrouvent des mutations récurrentes d’ESR1 essentiellement au niveau des
codons 537 et 538 de l’exon 8 en particulier chez des patientes traitées par AA. Dans
ces travaux, la fréquence estimée de mutations ESR1 acquises était comprise entre
20 et 50% pour des patientes présentant un cancer du sein métastatique avec un
taux de mutation très faible, voire nul, au sein de la tumeur primitive (0 à 3%). Sur le
plan fonctionnel, les mutations du gène ESR1 sont responsables d’une modification
conformationnelle du récepteur aux œstrogènes entrainant ainsi une activité de
transcription indépendante du ligand(17). A noter que les mutations situées au
niveau des codons 537 et 538 représentent 74% des mutations décrites (20). Les
mutations ESR1 sont ainsi le reflet d’une hormonorésistance(21) survenant sous
l’effet d’un traitement par AA en phase métastatique. Leur implication n’est
actuellement pas démontrée lors d’une hormonorésistance acquise sous
Tamoxifène(21).
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
1
/
43
100%