Clinical Diagnosis Video Transcript Cancer

1
PowerPoint Slides
English
European French Translation
Inflammatory Breast Cancer: Clinical Diagnosis
Video Transcript
Cancer inflammatoire du sein : le diagnostic clinique
Transcription de la vidéo
Professional Oncology Education
Inflammatory Breast Cancer: Clinical Diagnosis
Time: 13:25
Formation professionnelle d'oncologie
Cancer inflammatoire du sein : le diagnostic clinique
Durée : 13:25
Wendy A. Woodward, M.D., Ph.D.
Associate Professor,
Section Chief, Breast Radiation Oncology
Deputy Director, Morgan Welch Inflammatory
Breast Cancer Research Program and Clinic
The University of Texas MD Anderson Cancer
Center
Wendy A. Woodward, M.D., Ph.d.
Professeur associé,
Chef de section, radio-oncologie du sein
Directrice adjointe, clinique et programme de
recherche Morgan Welch sur le cancer
inflammatoire du sein
Centre du cancer MD Anderson de l'Université du
Texas
Hello, and welcome to The University of Texas MD
Anderson Cancer Center lecture s
eries on
Inflammatory Breast Cancer. In this section we’ll
discuss the clinical diagnosis of IBC. My name is
Wendy Woodward and I am a Radiation Oncologist
in the Breast Section here at MD Anderson.
Bonjour et bienvenue à la série de conférences sur
le cancer inflammatoire du sein au centre de cancer
MD Anderson de l'Université du Texas. Dans ce
volet, nous aborderons le diagnostic clinique du
CIS. Je suis Wendy Woodward et je suis oncologue
dans la clinique du sein, ici au MD Anderson.

2
Our goals over the course of this discussion are to be
sure that we can recognize the clinical presentation
of inflammatory breast cancer;
understand the
clinical definition; and identify common features.
Nos objectifs au cours de cette discussion seront :
découvrir le tableau clinique du cancer
inflammatoire du sein ; comprendre la définition
clinique ; et identifier les caractéristiques
communes.
We’ll begin with who is at risk. Demographic studies
of women who have inflammatory breast cancer
have demonstrated that this is largely a disease of
younger women, compared to non-inflammatory
breast cancer. In addition, demographic studies
have demonstrated an increase in the risk among
women from the Mediterranean area and North
Africa. Some of the limitations of studying a rare
disease like inflammatory breast cancer, however,
are that it’s difficult to validate risk factors and thus
far, there are indeed no validated risk factors that
could be used for screening. There is, however,
evidence that there is an increasing incidence in
inflammatory breast cancer and these are areas of
active research.
Nous commencerons par identifier les personnes à
risque. Les études démographiques des femmes
atteintes du cancer inflammatoire du sein ont
démontré que la maladie cible en grande partie les
jeunes femmes, en contraste avec le cancer du sein
non inflammatoire. En outre, des études
démographiques ont démontré une augmentation
du risque chez les femmes dans la région
Méditerranéenne et l'Afrique du Nord. L'étude d'une
maladie rare, comme le cancer inflammatoire du
sein, comporte cependant des limitations, il est ainsi
difficile de valider les facteurs de risque et jusqu'à
maintenant, ici, aucun facteur de risque qui pourrait
être utilisé pour le dépistage n’a été validé.
Toutefois, l’augmentation de l'incidence du cancer
inflammatoire du sein a été démontrée et des
recherches sont menées activement dans ces
domaines.

3
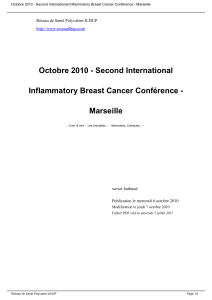
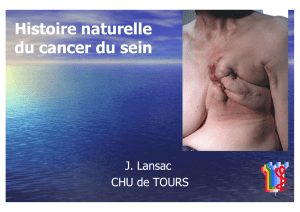
This is an age density histogram showing the age
distributions of patients with inflammatory and non-
inflammatory breast cancer. You can appreciate in
Panel A, looking at non-T4 breast cancer patients,
patients who have no disease involving the skin or
the chest wall, that there are two peaks in the age
density with the largest peak amongst older women
at 69 years of age. Amongst locally advanced breast
cancer patients, independent of their T4 status,
again, two peaks with a larger peak amongst older
women 74 years of age. This stands in contrast to
the distribution for inflammatory breast cancer
patients where the largest peak here is at 50 years of
age and really no second peak is demonstrated.
Voici un histogramme de densité selon l’âge des
patientes ; on peut y voir la répartition des patientes
atteintes du cancer du sein, inflammatoire et non
inflammatoire, selon l’âge. Dans la partie A, vous
pourrez observer les données correspondant aux
patientes atteintes d’un cancer non-T4, c’est à dire
des patientes dont la maladie n’implique ni la peau
ni la paroi thoracique. Il y a deux pics dans la
densité par âge, avec le pic le plus élevé parmi les
femmes âgées de 69 ans. Parmi les patientes
atteintes d’un cancer du sein localement avancé,
indépendamment de leur statut T4, nous avons à
nouveau deux pics dont le plus élevé se situe à l’
âge de 74 ans. Cela contraste avec la répartition
des patientes atteintes d’un cancer inflammatoire du
sein où le pic le plus élevé est à 50 ans et où nous
n’avons pas vraiment de deuxième pic.
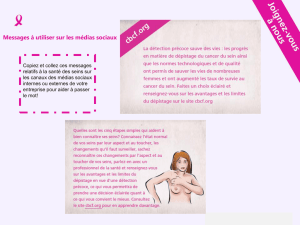
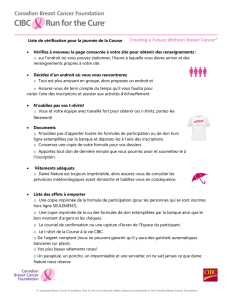
Looking in this population, the same authors, Hance
et al., were able to demonstrate that, in fact, the
incidence of inflammatory br
east cancer is
increasing. Here, looking from the early 1980s up
through 2000, you can see an increase in the
number of women per 100,000 woman/years. And
inflammatory breast cancer is going up at the same
time that the incidence of locally advanced breast
cancer is going down, likely through the benefits of
increased early screening. Interestingly, while there
has always been an increased incidence amongst
African-American women, particularly beginning in
the early 1980s and extending up through 2000, we
begin to see that white women are catching up in
terms of incidence with an increased incidence over
this time period.
En observant cette population, les mêmes
auteurs, Hance et al., ont pu démontrer qu’il y a en
réalité une augmentation de l'incidence du cancer
inflammatoire du sein. Ici, lorsqu’on étudie les
données du début des années 1980 jusqu’à l’année
2000, on observe une croissance, l’unité de mesure
étant dans ce cas 100 000 femmes par année. De
plus, le cancer inflammatoire du sein est en hausse
au même moment où l'incidence du cancer du sein
localement avancé diminue, sans doute grâce aux
avantages d’un dépistage précoce accru. Fait
intéressant : bien qu’il ait toujours eu une incidence
plus élevée chez les afro-américaines,
particulièrement depuis le début des années 1980
jusqu'en 2000, l’écart en termes d’incidence entre
les femmes afro-américaines et les femmes
blanches diminue et le taux d’incidence a augmenté
parmi les femmes blanches lors de cette même
période.

4
So “is this a new disease?” It certainly is not. The
clinical presentation of inflammatory breast cancer
was first described in 1814 by Sir Charles Bell, “A
purple color on the skin over the tumor accompanied
by shooting pains.” It was later then identified as
inflammatory breast cancer based on this visual
description, the symptoms that could be seen on the
breast. This is an important distinction because
“inflammatory” indicates to many that this is in fact a
response to an infection, but that’s a misnomer.
There is no clea
r evidence of the signs and
symptoms of infection, simply a breast cancer that
looks like infection.
Alors, « est-ce qu’il s’agit d’une nouvelle maladie? »
Certainement pas. Le tableau clinique du cancer
inflammatoire du sein a été décrit pour la première
fois en 1814 par Sir Charles Bell, « Une couleur
pourpre sur la peau au-dessus de la tumeur,
accompagnée de douleurs fulgurantes. » En se
basant sur la description visuelle et des symptômes
observés sur la poitrine, la maladie fut plus tard
identifiée comme le cancer inflammatoire du sein. Il
s'agit d'une distinction importante parce que le
terme « inflammatoire » signifie pour beaucoup la
réaction à une infection, l’appellation est en quelque
sorte un abus de langage. Il n'existe aucune preuve
claire des signes et symptômes d’une infection,
simplement un cancer du sein qui ressemble à une
infection.
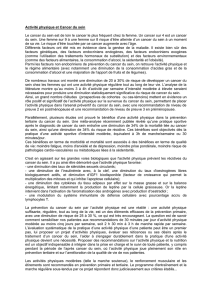
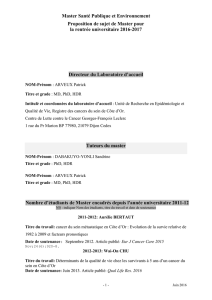
Here’s an example of the signs and symptoms of
inflammatory breast cancer. In particular there’s
erythema and breast edema that develops in a
previously normal breast. This can happen rapidly,
even overnight. Typically it will advance to involve
approximately two-thirds of the breast. The breast
can be tender; can have induration or warmth, or
peau d’orange, literally the skin of an orange.
Depicted here, you can appreciate that fluid and
swelling in the skin itself has caused the hair follicles
to stand out, making the skin appear orange-like.
This is a classic symptom of inflammatory breast
cancer. Because of the swelling and redness, this is
often diagnosed --- misdiagnosed as infection. It is
often not detected by mammogram, which adds to
this misdiagnotion --- misdiagnosis.
Voici un exemple des signes et symptômes du
cancer inflammatoire du sein. En particulier, nous
observons érythème et un œdème qui se
développent dans un/des sein/s qui se développent
dans un sein auparavant normal/aux. Cela peut se
produire rapidement, parfois même du jour au
lendemain. Ceci progressera en principe jusqu’à ce
que les deux tiers du sein soient touchés. Le sein
peut être sensible au toucher, se durcir ou donner
une sensation de chaleur, ou bien développer un
effet peau d'orange, littéralement comme la peau
d'une orange. Sur cette photo, vous pouvez
observer que les fluides et le gonflement de la peau
ont fait que les follicules pileux sont marqués, ce qui
rend la peau semblable à celle d’une orange. Ceci
est un symptôme classique du cancer inflammatoire
du sein. En raison du gonflement de la peau et des
rougeurs, ceci est souvent diagnostiqué à tort
comme une infection. Souvent, le cancer n’est pas
détecté par mammographie, ce qui contribue
également à ce diagnostic erroné.

5
An important distinction about inflammatory breast
cancer from non-inflammatory breast cancer is that it
is a clinical diagnosis. It’s not based on any specific
pathologic finding. So in the presence of the clinical
features we’ve just described and a biopsy proving
invasive breast cancer, the diagnosis of inflammatory
breast cancer can be made. In 2008, at the first
International Inflammat
ory Breast Cancer
Conference which was held here at MD Anderson
Cancer Center, a consensus panel of experts came
together to try and clarify the specific clinical
symptoms and signs which should lead to a
diagnosis of inflammatory breast cancer.
Specifically, a number of challenges were identified.
This is a relatively subjective diagnosis. “What is the
difference between one-third coverage of the breast
or two-thirds coverage of the breast?” “Is there clear
data exactly where this threshold should lie?” The
answer is “no”. Nevertheless, the authors and
participants of the Consensus Conference decided
that one-third of the breast would be the defining
characteristic over a time span of less than six
months. This indicates the rapid progression of
inflammatory breast cancer as we understand it as
well as the skin involvement. It is hallmark in
inflammatory breast cancer to find invasion of the
dermal lymphatics by tumor cells pathologically.
That’s depicted here. This, however, is not required
for the diagnosis of inflammatory breast cancer. You
must have a diagnosis of invasive disease but in the
absence of dermal lymphatic invasion but the
presence of clinical symptoms, this is still
inflammatory breast cancer.
Une distinction importante à faire quant au cancer
inflammatoire du sein en comparaison avec le
cancer du sein non inflammatoire, c'est qu'il s'agit
d'un diagnostic clinique. Il ne repose pas sur des
conclusions pathologiques spécifiques. Donc, en
présence des manifestations cliniques que nous
venons juste de décrire et d’une biopsie révélant un
cancer du sein invasif, le diagnostic du cancer
inflammatoire du sein peut être établi. En 2008, lors
de la première conférence internationale sur le
cancer inflammatoire du sein qui s'est tenue ici au
centre de cancer MD Anderson, un panel d'experts
s'est réuni pour tenter de clarifier les signes et les
symptômes cliniques spécifiques qui devraient
conduire à un diagnostic de cancer inflammatoire du
sein. Plus précisément, un certain nombre de défis
ont été identifiés. Il s'agit d'un diagnostic
relativement subjectif. « Quelle est la différence
entre le recouvrement d'un tiers du sein ou le
recouvrement des deux-tiers du sein ? » « Y a-t-il
des données exactes montrant où ce seuil doit être
défini ? » La réponse est « non ». Néanmoins, les
auteurs et les participants à la conférence de
consensus ont tranché sur la caractéristique
déterminante et l’ont fixé à un tiers du sein sur une
période de moins de six mois. Cela indique la
progression rapide du cancer inflammatoire du sein
comme nous le comprenons, ainsi que l'implication
de la peau. Une caractéristique distincte dans le
cancer inflammatoire du sein est de découvrir une
invasion pathologique des vaisseaux lymphatiques
cutanés par des cellules tumorales. Ce qui est
représenté ici. Ce n'est toutefois pas requis pour le
diagnostic du cancer inflammatoire du sein. Vous
devez avoir un diagnostic de maladie invasive, mais
en l'absence d'invasion lymphatique cutanée, la
présence de symptômes cliniques suffit pour
déterminer qu’il s'agit du cancer inflammatoire du
sein.
 6
7
8
9
10
11
12
13
6
7
8
9
10
11
12
13
1
/
13
100%