Quand débuter les antirétroviraux? Recommandations

Quand débuter les antirétroviraux?
Recommandations internationales
Formation à l’usage des
antirétroviraux
Pr Willy Rozenbaum


clinicaloptions.com/hiv
When to Start Antiretroviral Therapy
Potential Benefits of Early Therapy
Earlier suppression of viral replication
Preservation of immune function
Prolongation of disease-free survival
Lower risk of virologic failure?
Lower risk of detrimental viral evolution
Possible decrease in the risk of HIV transmission

clinicaloptions.com/hiv
When to Start Antiretroviral Therapy
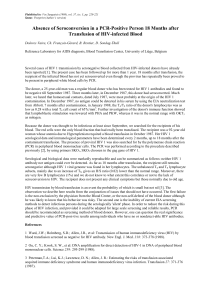
CD4+ Cell Count Response Based on
Baseline CD4+ Cell Count
Keruly J, et at. CROI 2006. Abstract 529.
Gras L, et al. CROI 2006. Abstract 530.
048 96 144 192 240 288 336
Years on HAART
ATHENA National Cohort
Johns Hopkins HIV Clinical Cohort
Mean CD4+ Cell Count
(cells/mm3)
200
400
600
800
0
01 2 3 4 5
Weeks From Starting HAART
1000
200
400
600
800
0
1000
> 500
351-500
201-350
51-200
< 50
BL CD4
> 350
< 200
201-350
BL CD4

clinicaloptions.com/hiv
When to Start Antiretroviral Therapy
101-200 cells/mm3
201-350 cells/mm3
351-500 cells/mm3
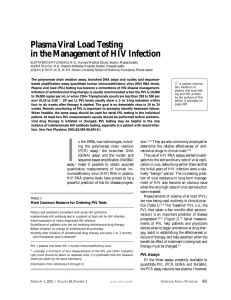
HAART and Survival Based on Initial
CD4+ Cell Count
Modeled data from ART Cohort
Collaborative
10,855 patients included
934 progressed to AIDS or died
IDUs censored from model
D’Arminio Monforte A, et al. CROI 2006. Abstract 525.
Cumulative Probability of AIDS/Death According
to CD4+ Cell Count at Initiation of HAART
Years Since Initiation of HAART
01 2 34 5
0.00
0.02
0.04
0.06
0.08
0.10
0.12
Probability of AIDS or Death
0.14
Progression and Death According
to CD4+ Cell Count (cells/mm3)
< 200 vs
201-350 < 350 vs
351-500
Hazard ratio for
AIDS (95% CI) 3.68
(3.01-4.51) 1.52
(1.10-2.10)
Hazard ratio for
AIDS or death
(95% CI)
2.93
(2.41-3.57) 1.26
(0.94-1.68)
 6
7
8
9
6
7
8
9
1
/
9
100%